

Early and Sustained Symptom Control with Mirikizumab in Patients with Ulcerative Colitis in the Phase 3 LUCENT Programme
- PMID: 38869019
- PMCID: PMC11532612
- DOI: 10.1093/ecco-jcc/jjae088
Early and Sustained Symptom Control with Mirikizumab in Patients with Ulcerative Colitis in the Phase 3 LUCENT Programme
Abstract
Background and aims: Ulcerative colitis [UC], a chronic inflammatory bowel disease, may manifest with symptoms of increased stool frequency [SF], rectal bleeding [RB], bowel urgency [BU], abdominal pain [AP], and fatigue. Mirikizumab, an anti-IL-23p19 antibody, demonstrated efficacy and safety in patients with moderately to severely active UC in the LUCENT Phase 3 trials. We evaluated mirikizumab's efficacy in achieving symptom control and time to symptom improvement during induction, maintenance of sustained symptom control, 'comprehensive symptom control', defined according to a combination of individual patient-reported outcomes, and prognostic baseline indicators of early symptomatic remission at Week 4.
Methods: The results of LUCENT-1/-2 have previously been reported. Treatment differences for symptomatic endpoints were compared over 52 weeks versus placebo [PBO] and comprehensive symptomatic endpoints at 12 and 52 weeks of continuous treatment. Subgroup analyses were conducted for prior biologic or tofacitinib treatment failure. Prognostic analyses were run using regression analysis.
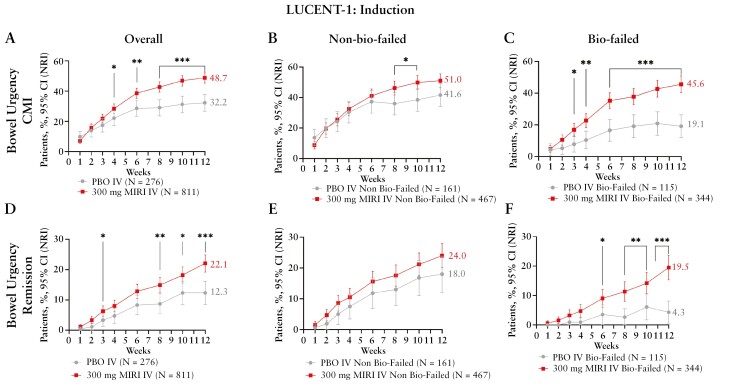
Results: By Week [W] 2, mirikizumab-treated patients achieved greater reductions in SF, RB, BU, and fatigue versus PBO. At W4, there was a higher rate of AP improvement. At W12, a greater proportion of mirikizumab-treated patients achieved symptomatic remission, RB remission, SF remission, and BU remission/clinically meaningful improvement. Mirikizumab-treated patients sustained symptom control versus placebo patients in maintenance until W52. This treatment effect was shown in patients regardless of prior biologic or tofacitinib failure. Additionally, mirikizumab achieved comprehensive symptom control versus PBO at W12 and W52.
Conclusions: Mirikizumab demonstrated efficacy in achieving and sustaining symptom control and comprehensive symptom control over 52 weeks [NCT03518086; NCT03524092].
Keywords: Comprehensive; symptom; ulcerative colitis.
© The Author(s) 2024. Published by Oxford University Press on behalf of European Crohn’s and Colitis Organisation.
Conflict of interest statement
SD reports consultancy fees from AbbVie, Alimentiv, Allergan, Amgen, Applied Molecular Transport, AstraZeneca, Athos Therapeutics, Biogen, Boehringer Ingelheim, Bristol Myers Squibb, Celgene, Celltrion, Dr Falk Pharma, Eli Lilly and Company, Enthera, Ferring Pharmaceuticals, Gilead, Hospira, Inotrem, Janssen, Johnson & Johnson, Morphic, MSD, Mundipharma, Mylan, Pfizer, Roche, Sandoz, Sublimity Therapeutics, Takeda, Teladoc Health, TiGenix, UCB, Vial, Vifor; lecture fees from AbbVie, Amgen, Ferring Pharmaceuticals, Gilead, Janssen, Mylan, Pfizer, Takeda. AD reports fees for participation in clinical trials and review activities such as data monitoring boards, statistical analysis, and endpoint committees from Abivax, AbbVie, Arena Pharmaceuticals, Bristol Myers Squibb/Celgene, Dr Falk Foundation, Galapagos, Gilead, Janssen, and Pfizer; consultancy fees from AbbVie, Amgen, Arena Pharmaceuticals, Biogen, Boehringer Ingelheim, Bristol Myers Squibb/Celgene, Celltrion, Dr Falk Foundation, Ferring Pharmaceuticals, Fresenius Kabi, Galapagos, Janssen, Lilly, MSD, Pfizer, Pharmacosmos, Roche/Genentech, Sandoz/Hexal, Takeda, Tillotts, and Vifor Pharma; payment from lectures, including service on speakers’ bureaus, from AbbVie, Biogen, CED Service GmbH, Celltrion, Falk Foundation, Ferring, Galapagos, Gilead, High5MD, Janssen, Materia Prima, MedToday, MSD, Pfizer, Streamed-Up, Takeda, Tillotts, and Vifor Pharma; payment for manuscript preparation from Falk Foundation, Takeda, Thieme, and UniMed. KM received research grants from AbbVie, Mochida, Nippon Kayaku, Zeria, and JIMRO; speakers’ fees from Eli Lilly and Company, Mitsubishi Tanabe Pharma, Takeda, Janssen, AbbVie, EA Pharma, Pfizer, Takeda, Mochida, Kyorin, Zeria, Kissei, Gilead Scientific, Nippon Kayaku, and Celltrion. MF received research grants from AbbVie, Amgen, Biogen, EG, Janssen, Pfizer, Takeda, and Viatris; consultancy fees from AbbVie, AgomAb Therapeutics, Boehringer Ingelheim, Celgene, Celltrion, Eli Lilly and Company, Janssen-Cilag, Medtronic, MRM Health, MSD, Pfizer, Regeneron, Samsung Bioepis, Sandoz, Takeda, and ThermoFisher; and speakers’ fees from AbbVie, Amgen, Biogen, Boehringer Ingelheim, Falk, Ferring, Janssen-Cilag, Lamepro, MSD, Pfizer, Sandoz, Takeda, Truvion Healthcare, and Viatris. ML has served as a consultant for AbbVie, Pfizer, Takeda, Lilly, Bristol-Meyers Squibb, Target RWE, and Prometheus; and has received research support from Pfizer, Takeda, and Janssen. IS, RM, SM, THG, and NM are employees of Eli Lilly and Company. CM was an employee of Eli Lilly and Company during the design, conduct, and analyses of the clinical studies. MTA has received research funding from the National Institute of Health, Department of Defense, charities including the Leona M. and Harry B. Helmsley Charitable Trust, Crohn’s and Colitis Foundation, and Kenneth Rainin Foundation; is a consultant or served on advisory boards for AbbVie, Arena Pharmaceuticals [now Pfizer], Bristol Myers Squibb, Celsius Therapeutics, Eli Lilly and Company, Gilead Sciences, Janssen Pharmaceuticals, Janssen Global Services, Pfizer Pharmaceutical, Prometheus Biosciences, and UCB Biopharma SRL; has received fees for lecturing from Alimentiv, Janssen Pharmaceuticals, Prime CME, and WebMD Global LLC.
Figures





References
-
- Ordas I, Eckmann L, Talamini M, Baumgart DC, Sandborn WJ.. Ulcerative colitis. Lancet 2012;380:1606–19. - PubMed
-
- Dubinsky MC, Irving PM, Panaccione R, et al. Incorporating patient experience into drug development for ulcerative colitis: development of the urgency numeric rating scale, a patient-reported outcome measure to assess bowel urgency in adults. Journal of Patient-Reported Outcomes 2022;6:31. - PMC - PubMed
-
- Sandborn WJ, Feagan BG, Loftus EV Jr, et al. Efficacy and safety of upadacitinib in a randomised trial of patients with Crohn’s disease. Gastroenterology 2020;158:2123–38.e8. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
