

Age-specific Multimorbidity Patterns and Burden on All-Cause Mortality and Public Direct Medical Expenditure: A Retrospective Cohort Study
- PMID: 38869775
- PMCID: PMC11444029
- DOI: 10.1007/s44197-024-00256-y
Age-specific Multimorbidity Patterns and Burden on All-Cause Mortality and Public Direct Medical Expenditure: A Retrospective Cohort Study
Abstract
Objective: To evaluate age-specific multimorbidity patterns and morbidity burden on mortality and healthcare expenditure across age groups.
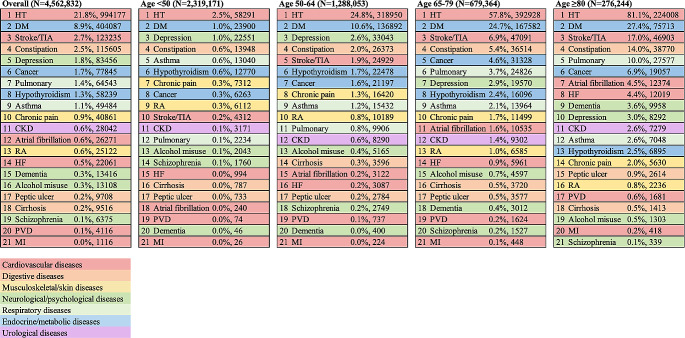
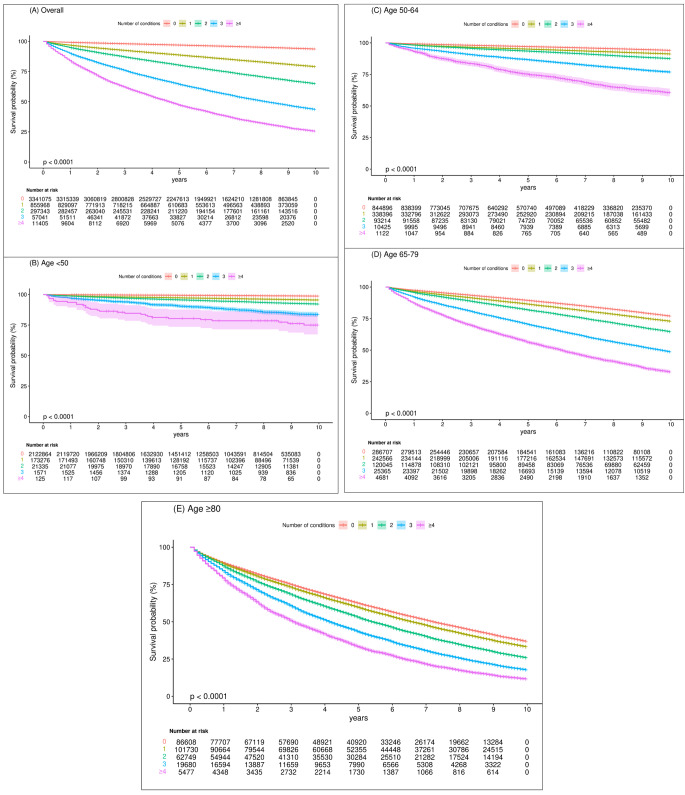
Patients and methods: Retrospective observational study between January 1, 2009 to December 31, 2017 using electronic health records in Hong Kong: Individuals were stratified by age (< 50, 50-64, 65-79, ≥ 80), and sub-classified by number of morbidities (0, 1, 2, 3, ≥ 4) out of 21 common chronic conditions. Clustering analyses were conducted to identify specific patterns of multimorbidity. Association between the number as well as combinations of morbidities and all-cause mortality and public expenditure was examined.
Results: 4,562,832 individuals with a median follow-up of 7 years were included. Mental disorders were the top morbidities among young individuals, while cardiovascular diseases were prevalent in the elderly. An increased number of morbidities was associated with a greater relative risk for mortality and medical expenditure, and this relationship was stronger among younger patients. Compared to individuals in the same age group without morbidity, the hazard ratios (HR; 95% CI) of all-cause mortality in patients aged < 50 and ≥ 80 with two comorbidities 3.81 (3.60-4.03) and 1.38 (1.36-1.40), respectively, which increased to 14.22 (9.87-20.47) and 2.20 (2.13-2.26), respectively, as the number of morbidities increased to ≥ 4. The stroke-hypertension cluster was shown to be associated with the highest HR of mortality 2.48 (2.43-2.53) among all identified clusters arising from the clustering analysis.
Conclusion: Given the stronger association between multimorbidity and all-cause mortality and greater opportunity costs in younger populations, prevention and management of early-onset multimorbidity are warranted. (248 words).
Keywords: All-cause mortality; Healthcare expenditure; Multimorbidity; Observational study.
© 2024. The Author(s).
Conflict of interest statement
Competing Interests FTTL has been supported by the RGC Postdoctoral Fellowship under the Hong Kong Research Grants Council and has received research grants from the Food and Health Bureau of the Government of the Hong Kong Special Administrative Region, outside the submitted work. ICKW reports research funding from Amgen, Bristol Myers Squibb, Pfizer, Janssen, Bayer, GSK, Novartis, the Hong Kong Research Grants Council, the Hong Kong Health and Medical Research Fund, the National Institute for Health Research in England, the European Commission, and the National Health and Medical Research Council in Australia, outside the submitted work; and is a non-executive director of Jacobson Medical in Hong Kong and a consultant to IQVIA and World Health Organization. EYFW has received research grants from the Food and Health Bureau of the Government of the Hong Kong Special Administrative Region, the Hong Kong Research Grants Council of the Government of the Hong Kong SAR, Narcotics Division, Security Bureau of the Government of the Hong Kong SAR, and National Natural Science Foundation of China, outside the submitted work. All other authors declare no competing interests.
Figures

Similar articles
-
Age-specific associations between the number of co-morbidities, all-cause mortality and public direct medical costs in patients with type 2 diabetes: A retrospective cohort study.Diabetes Obes Metab. 2023 Feb;25(2):454-467. doi: 10.1111/dom.14889. Epub 2022 Nov 2. Diabetes Obes Metab. 2023. PMID: 36205484
-
Catastrophic out-of-pocket payments related to non-communicable disease multimorbidity and associated factors, evidence from a public referral hospital in Addis Ababa Ethiopia.BMC Health Serv Res. 2024 Aug 6;24(1):896. doi: 10.1186/s12913-024-11392-3. BMC Health Serv Res. 2024. PMID: 39107740 Free PMC article.
-
Multimorbidity and Its Outcomes Among Patients Attending Psychiatric Care Settings: An Observational Study From Odisha, India.Front Public Health. 2021 Apr 21;8:616480. doi: 10.3389/fpubh.2020.616480. eCollection 2020. Front Public Health. 2021. PMID: 33968863 Free PMC article.
-
The association between multimorbidity and out-of-pocket expenditure for prescription medicines among adults in Denmark: A population-based register study.Res Social Adm Pharm. 2025 Jul;21(7):549-558. doi: 10.1016/j.sapharm.2025.03.009. Epub 2025 Mar 17. Res Social Adm Pharm. 2025. PMID: 40121125
-
The role of mental disease on the association between multimorbidity and medical expenditure.Fam Pract. 2020 Sep 5;37(4):453-458. doi: 10.1093/fampra/cmaa015. Fam Pract. 2020. PMID: 32086514
Cited by
-
Age-Related Variations and Seasonal Influences: A Network Analysis of Comorbidities in Asthma Hospitalizations (2013-2023).J Clin Med. 2025 Mar 29;14(7):2350. doi: 10.3390/jcm14072350. J Clin Med. 2025. PMID: 40217800 Free PMC article.
-
Extrahepatic disease clusters and mortality in people with steatotic liver diseases: a prospective analysis of 64,749 females and 113,587 males in the UK Biobank.BMC Med. 2025 Jul 31;23(1):450. doi: 10.1186/s12916-025-04288-4. BMC Med. 2025. PMID: 40745309 Free PMC article.
-
Identifying multimorbidity risks in older adults: a cross-sectional study using the RGA screening data.Front Public Health. 2025 Jul 28;13:1600779. doi: 10.3389/fpubh.2025.1600779. eCollection 2025. Front Public Health. 2025. PMID: 40791623 Free PMC article.
References
-
- Nunes BP, Flores TR, Mielke GI, Thumé E, Facchini LA. Multimorbidity and mortality in older adults: a systematic review and meta-analysis. Arch Gerontol Geriatr. 2016;67:130–8. - PubMed
-
- Marengoni A, Rizzuto D, Wang HX, Winblad B, Fratiglioni L. Patterns of chronic multimorbidity in the elderly population. J Am Geriatr Soc. 2009;57:225–30. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
