

A Phase II Study of Potentiation of Pembrolizumab with Binimetinib and Bevacizumab in Refractory Microsatellite-Stable Colorectal Cancer
- PMID: 38869830
- PMCID: PMC11369619
- DOI: 10.1158/1078-0432.CCR-24-0090
A Phase II Study of Potentiation of Pembrolizumab with Binimetinib and Bevacizumab in Refractory Microsatellite-Stable Colorectal Cancer
Abstract
Purpose: In this single-institution phase II investigator-initiated study, we assessed the ability of MAPK and VEGF pathway blockade to overcome resistance to immunotherapy in microsatellite-stable metastatic colorectal cancer (MSS mCRC).
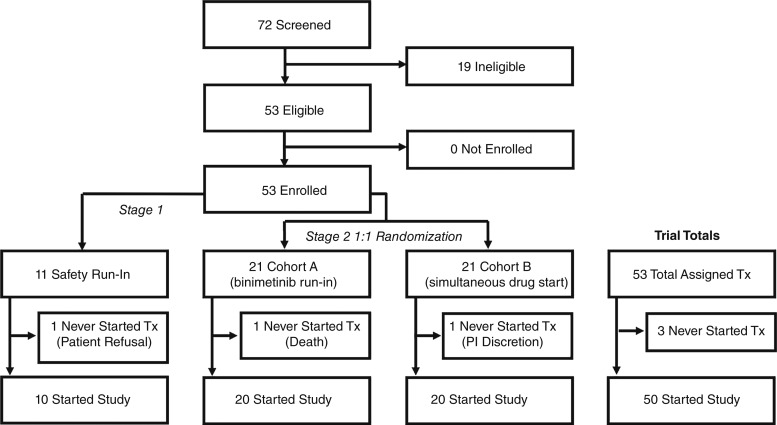
Patients and methods: Patients with MSS, BRAF wild-type mCRC who progressed on ≥2 prior lines of therapy received pembrolizumab, binimetinib, and bevacizumab until disease progression or unacceptable toxicity. After a safety run-in, patients were randomized to a 7-day run-in of binimetinib or simultaneous initiation of all study drugs, to explore whether MEK inhibition may increase tumor immunogenicity. The primary endpoint was objective response rate (ORR) in all patients combined (by Response Evaluation Criteria in Solid Tumors v1.1).
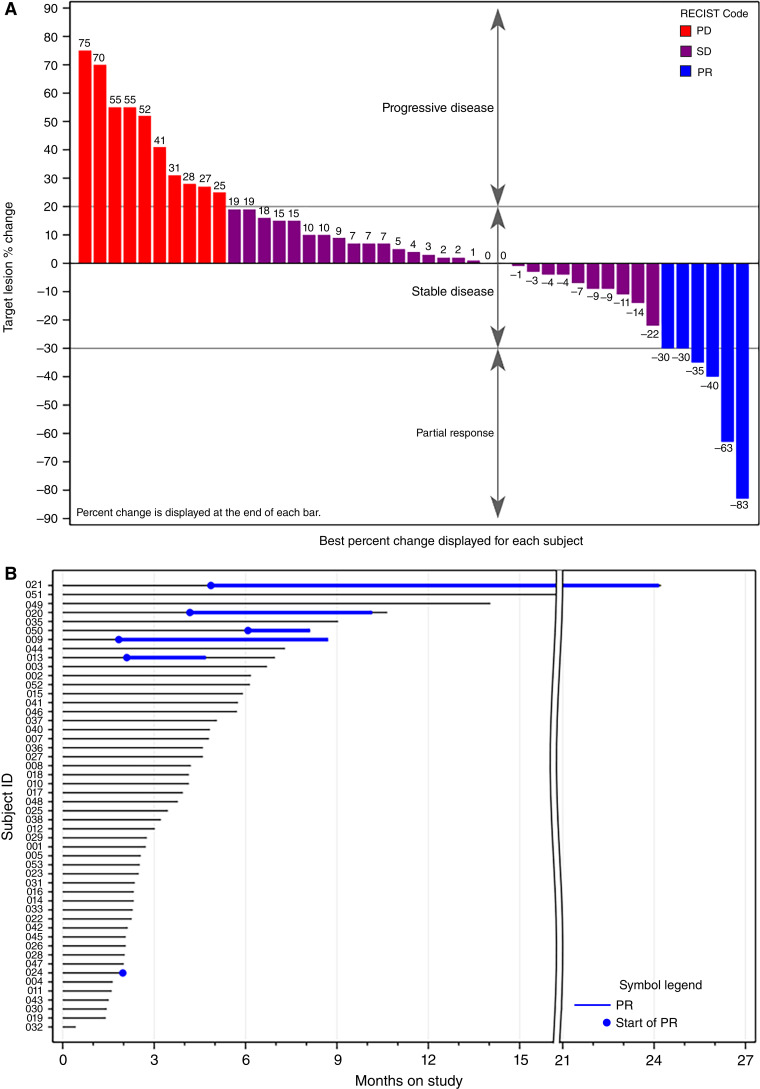
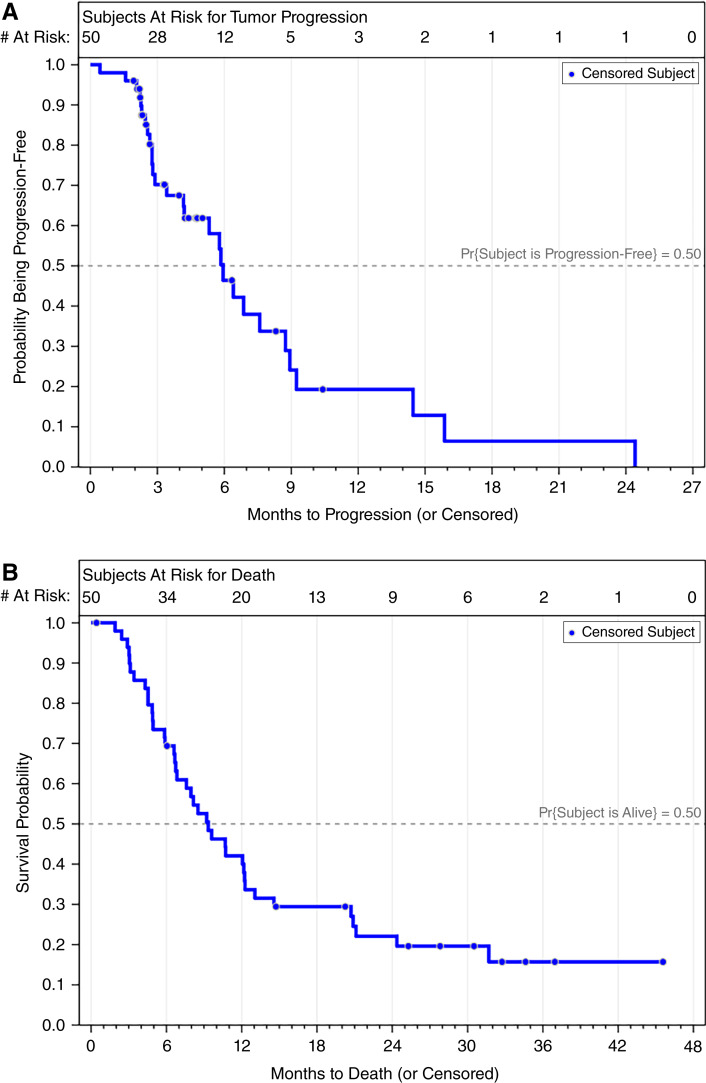
Results: Fifty patients received study drug treatment; 54% were male with a median age of 55 years (range, 31-79). The primary endpoint, ORR, was 12.0% [95% confidence interval (CI) 4.5%-24.3%], which was not statistically different than the historical control data of 5% (P = 0.038, exceeding prespecified threshold of 0.025). The disease control rate was 70.0% (95% CI, 55.4%-82.1%), the median progression-free survival 5.9 months (95% CI, 4.2-8.7 months), and the median overall survival 9.3 months (95% CI, 6.7-12.2 months). No difference in efficacy was observed between the randomized cohorts. Grade 3 and 4 adverse events were observed in 56% and 8% of patients, respectively; the most common were rash (12%) and increased aspartate aminotransferase (12%).
Conclusions: Pembrolizumab, binimetinib, and bevacizumab failed to meet its primary endpoint of higher ORR compared with historical control data, demonstrated a high disease control rate, and demonstrated acceptable tolerability in refractory MSS mCRC.
©2024 The Authors; Published by the American Association for Cancer Research.
Conflict of interest statement
R.W. Lentz reports grants from NIH during the conduct of the study; R.W. Lentz also reports grants from ALX Oncology, Guardant, and EDDC; nonfinancial support from Merck and Eli Lilly and Company; other support from Myeloid Therapeutics and Agenus; and grants and other support from Boehringer Ingelheim outside the submitted work. T.M. Pitts reports grants from NIH during the conduct of the study. S.L. Davis reports other support from Merck during the conduct of the study, as well as other support from Bristol Myers Squibb, Symphogen, I-Mab, TriSalus Life Sciences, Tvardi Therapeutics, EMD Serono, and ORIC Pharmaceuticals outside the submitted work. S.S. Kim reports grants from Merck and other support from Eisai, Bristol Myers Squibb, Daiichi Sankyo, and Astellas outside the submitted work. A.D. Leal reports nonfinancial support and other support from Bristol Myers Squibb and Exelixis; nonfinancial support from Elicio Therapeutics, Inc., AbbVie, FameWave Ltd., Conjupro Biotherapeutics, Inc., and Corcept Therapeutics; and other support from Elsevier outside the submitted work. S.G. Eckhardt reports other support from Exelixis, Amgen, and OnKure outside the submitted work. C.H. Lieu reports grants from NCI R01CA229259-01, Merck, and Pfizer during the conduct of the study. No disclosures were reported by the other authors.
Figures
References
-
- Siegel RL, Miller KD, Wagle NS, Jemal A. Cancer statistics, 2023. CA Cancer J Clin 2023;73:17–48. - PubMed
-
- Douillard JY, Siena S, Cassidy J, Tabernero J, Burkes R, Barugel M, et al. . Randomized, phase III trial of panitumumab with infusional fluorouracil, leucovorin, and oxaliplatin (FOLFOX4) versus FOLFOX4 alone as first-line treatment in patients with previously untreated metastatic colorectal cancer: the PRIME study. J Clin Oncol 2010;28:4697–705. - PubMed
-
- Douillard JY, Oliner KS, Siena S, Tabernero J, Burkes R, Barugel M, et al. . Panitumumab-FOLFOX4 treatment and RAS mutations in colorectal cancer. N Engl J Med 2013;369:1023–34. - PubMed
-
- Di Nicolantonio F, Martini M, Molinari F, Sartore-Bianchi A, Arena S, Saletti P, et al. . Wild-type BRAF is required for response to panitumumab or cetuximab in metastatic colorectal cancer. J Clin Oncol 2008;26:5705–12. - PubMed
-
- Mayer RJ, Van Cutsem E, Falcone A, Yoshino T, Garcia-Carbonero R, Mizunuma N, et al. . Randomized trial of TAS-102 for refractory metastatic colorectal cancer. N Engl J Med 2015;372:1909–19. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
