

Circulating Tumor DNA-Guided De-Escalation Targeted Therapy for Advanced Non-Small Cell Lung Cancer: A Nonrandomized Controlled Trial
- PMID: 38869865
- PMCID: PMC12312504
- DOI: 10.1001/jamaoncol.2024.1779
Circulating Tumor DNA-Guided De-Escalation Targeted Therapy for Advanced Non-Small Cell Lung Cancer: A Nonrandomized Controlled Trial
Abstract
Importance: Uninterrupted targeted therapy until disease progression or intolerable toxic effects is currently the routine therapy for advanced non-small cell lung cancer (NSCLC) involving driver gene variations. However, drug resistance is inevitable.
Objective: To assess the clinical feasibility of adaptive de-escalation tyrosine kinase inhibitor (TKI) treatment guided by circulating tumor DNA (ctDNA) for achieving complete remission after local consolidative therapy (LCT) in patients with advanced NSCLC.
Design, setting, and participants: This prospective nonrandomized controlled trial was conducted at a single center from June 3, 2020, to July 19, 2022, and included 60 patients with advanced NSCLC with driver variations without radiologically detectable disease after TKI and LCT. The median (range) follow-up time was 19.2 (3.8-29.7) months. Data analysis was conducted from December 15, 2022, to May 10, 2023.
Intervention: Cessation of TKI treatment and follow-up every 3 months. Treatment was restarted in patients with progressive disease (defined by the Response Evaluation Criteria in Solid Tumors 1.1 criteria), detectable ctDNA, or elevated carcinoembryonic antigen (CEA) levels, whichever manifested first, and treatment ceased if all indicators were negative during follow-up surveillance.
Main outcomes and measures: Progression-free survival (PFS). Secondary end points were objective response rate, time to next treatment, and overall survival.
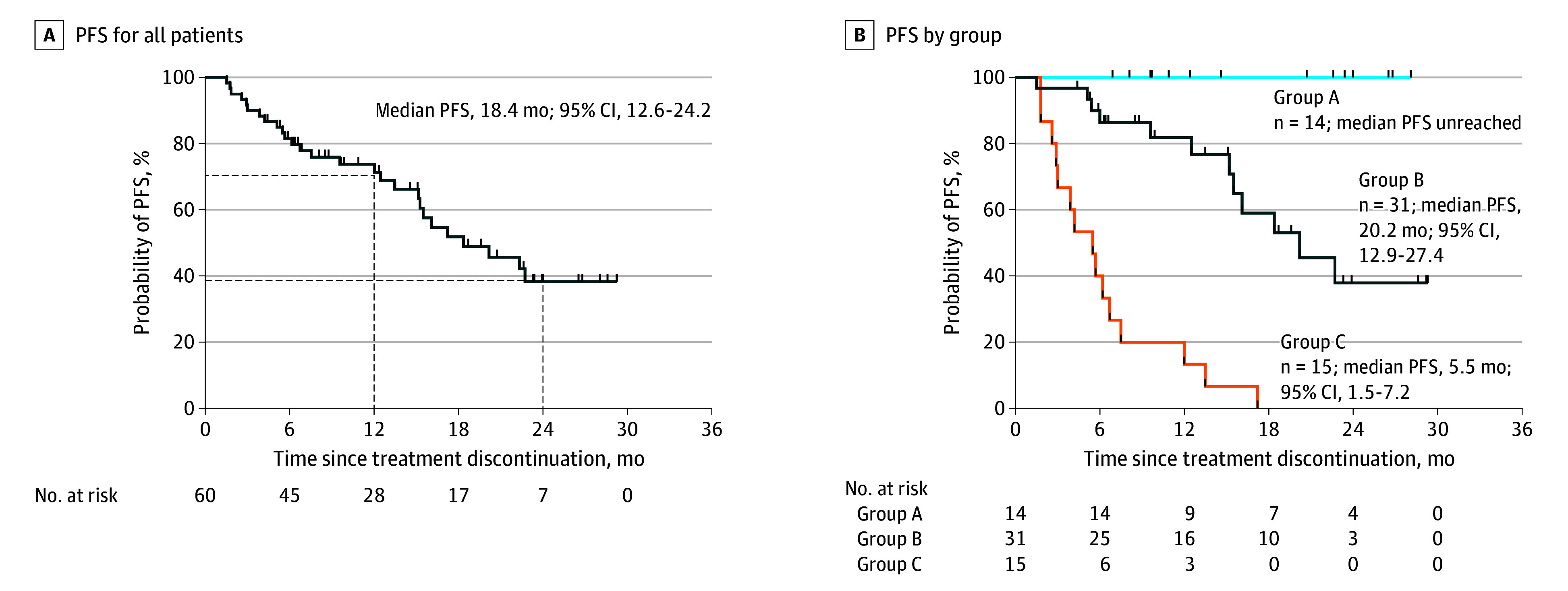
Results: Among the total study sample of 60 participants (median [range] age, 55 [21-75] years; 33 [55%] were female), the median PFS was 18.4 (95% CI, 12.6-24.2) months and the median (range) total treatment break duration was 9.1 (1.5-28.1) months. Fourteen patients (group A) remained in TKI cessation with a median (range) treatment break duration of 20.3 (6.8-28.1) months; 31 patients (group B) received retreatment owing to detectable ctDNA and/or CEA and had a median PFS of 20.2 (95% CI, 12.9-27.4) months with a median (range) total treatment break duration of 8.8 (1.5-20.6) months; and 15 patients (group C) who underwent retreatment with TKIs due to progressive disease had a median PFS of 5.5 (95% CI, 1.5-7.2) months. For all participants, the TKI retreatment response rate was 96%, the median time to next treatment was 29.3 (95% CI, 25.3-35.2) months, and the data for overall survival were immature.
Conclusions and relevance: The findings of this nonrandomized controlled trial suggest that this adaptive de-escalation TKI strategy for patients with NSCLC is feasible in those with no lesions after LCT and a negative ctDNA test result. This might provide a de-escalation treatment strategy guided by ctDNA for the subset of patients with advanced NSCLC.
Trial registration: ClinicalTrials.gov Identifier: NCT03046316.
Conflict of interest statement
Figures



Comment in
-
Can circulating tumor DNA guide treatment de-escalation in metastatic lung adenocarcinoma harboring actionable genomic alterations?Transl Lung Cancer Res. 2024 Dec 31;13(12):3831-3834. doi: 10.21037/tlcr-24-861. Epub 2024 Dec 24. Transl Lung Cancer Res. 2024. PMID: 39830755 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
