

Adaptive Steroid Tapering Impedes Corticosteroid-free Remissions Compared with Forced Tapering in Clinical Trials of Ulcerative Colitis
- PMID: 38869911
- PMCID: PMC11532608
- DOI: 10.1093/ecco-jcc/jjae092
Adaptive Steroid Tapering Impedes Corticosteroid-free Remissions Compared with Forced Tapering in Clinical Trials of Ulcerative Colitis
Abstract
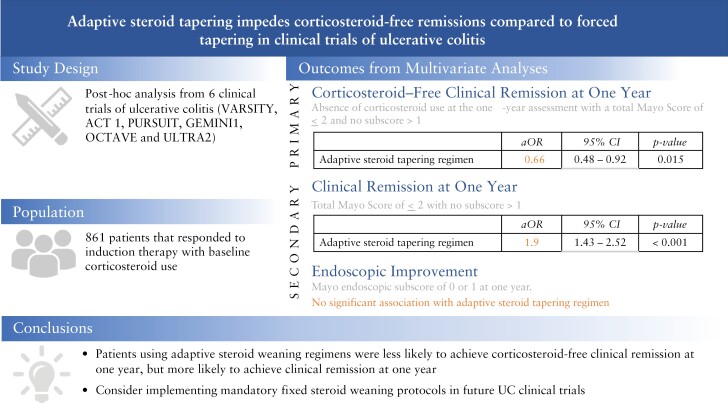
Introduction: It is unclear if steroid tapering protocols can affect clinical trial outcomes in ulcerative colitis [UC], particularly fixed versus adaptive steroid tapering. Fixed steroid tapering involves incremental dose decreases at prespecified intervals, and adaptive steroid tapering uses investigator discretion as determined by the patient's response.
Methods: In this post-hoc analysis from six clinical trials of UC [VARSITY, ACT 1, PURSUIT, GEMINI1, OCTAVE, and ULTRA2], responders to induction therapy with baseline corticosteroid use were considered as the primary population of interest. Adjustments were made to account for treat-through versus re-randomisation designs, and multivariate regression was performed to account for other potential confounding variables. The primary outcome was corticosteroid-free clinical remission [CR] at 1 year, and secondary outcomes were CR and endoscopic improvement.
Results: There was a total of 861 patients who had achieved clinical response after induction and were using corticosteroids. Within multivariate analysis, patients using adaptive steroid tapering regimens were less likely to achieve corticosteroid-free CR at 1 year (odds ratio [OR] 0.66 [95% confidence interval, CI, 0.48-0.92], p = 0.015) but had increased odds for achieving CR at 1 year (OR 1.9 [95% CI 1.43-2.52], p < 0.001). The steroid tapering regimen was not associated with achievement of endoscopic improvement at 1 year.
Conclusions: Among patients with UC on corticosteroids in clinical trials, patients using adaptive steroid weaning regimens were less likely to achieve corticosteroid-free CR at 1 year but more likely to achieve CR at 1 year. Consideration should be given to implementing mandatory fixed steroid weaning protocols in future clinical trials of UC.
Keywords: Corticosteroid; steroid; ulcerative colitis; weaning.
© The Author(s) 2024. Published by Oxford University Press on behalf of European Crohn’s and Colitis Organisation.
Conflict of interest statement
NN has received honoraria from Janssen, Abbvie, Takeda, Pfizer, Sandoz, Novartis, Iterative Health, Innomar Strategies, Fresinius Kabi, Amgen, Organon, Eli Lilly, and Ferring. PSD has received research support, consulting, and/or speaker fees from Abbvie, Abivax, Adiso, Bristol Meyers Squibb, GSK, Janssen, Lilly, Pfizer, Roivant, Takeda; and royalties from University of California San Diego. JKM has receive consulting and/or speaking fees from AbbVie, Alimentiv, Amgen, Astra Zeneca, Bausch Health, Bristol Myers Squibb, Celltrion, Ferring, Fresenius Kabi, Janssen, Lilly, Lupin, Organon, Paladin, Pfizer, Pharmascience, Qu Biologics, Roche, Sandoz, SCOPE, Takeda, Teva, Viatris. WR has served as a speaker for AbbVie, Celltrion, Falk Pharma GmbH, Ferring, Janssen, Galapagos Medice, MSD, Roche, Pfizer, Pharmacosmos, Shire, Takeda, Therakos; as a consultant for AbbVie, Amgen, AOP Orphan, Arena Pharmaceuticals, Astellas, Astra Zeneca, Bioclinica, Boehringer Ingelheim, Bristol Myers Squibb, Calyx, Celgene, Celltrion, Eli Lilly, Falk Pharma GmbH, Ferring, Galapagos, Gatehouse Bio, Genentech, Gilead, Grünenthal, ICON, Index Pharma, Inova, Janssen, Landos Biopharma, Medahead, MedImmune, Microbiotica, Mitsubishi Tanabe Pharma Corporation, MSD, Novartis, OMass, Otsuka, Parexel, Periconsulting, Pharmacosmos, Pfizer, Protagonist, Provention, Quell Therapeutics, Sandoz, Seres Therapeutics, Setpointmedical, Sigmoid, Sublimity, Takeda, Teva Pharma, Therakos, Theravance, Zealand; as an advisory board member for AbbVie, Amgen, Astra Zeneca, Boehringer Ingelheim, Bristol Myers Squibb, Celgene, Celltrion, Galapagos, Janssen, Mitsubishi Tanabe Pharma Corporation, MSD, Pharmacosmos, Pfizer, Sandoz, Takeda; and has received research funding from AbbVie, Janssen, MSD, Sandoz, Sanofi, Takeda. VJ has received consulting/advisory board fees from AbbVie, Alimentiv, Arena Pharmaceuticals, Asahi Kasei Pharma, Asieris, Astra Zeneca, Avoro Capital, Bristol Myers Squibb, Celltrion, Eli Lilly, Endpoint Health, Enthera, Ferring, Flagship Pioneering, Fresenius Kabi, Galapagos, Gilde Healthcare, GlaxoSmithKline, Genentech, Gilead, Innomar, JAMP, Janssen, Merck, Metacrine, Mylan, Pandion, Pendopharm, Pfizer, Protagonist, Prometheus Biosciences, Reistone Biopharma, Roche, Roivant, Sandoz, SCOPE, Second Genome, Sorriso, Takeda, TD Securities, Teva, Topivert, Ventyx, Vividion; speaker’s fees from Abbvie, Ferring, Bristol Myers Squibb, Galapagos, Janssen Pfizer Shire, Takeda, Fresenius Kabi. SBH declares potential conflicts of interest including: Abbvie consultant, Clinical Research [Institution], speaker,; Amgen consultant, Clinical Research [Institution]; Boehringer-Ingelheim consultant; BMS consultant, DSMB; Celltrion consultant; Fresnius-Kabi consultant; Genentech consultant, Clinical Research, [Institution]; Gilead consultant, Clinical Research [Institution]; Gossamer DSMB, GSK consultant, Clinical Research [Institution]; Immunic consultant; Intercept Pharmaceiticals; Janssen consultant, Clinical Research [Institution], speaker; Lilly consultant, Clinical Research [Institution]; Merck consultant; Novartis consultant, Clinical Research [Institution]; Organon consultant; Pfizer consultant, Clinical Research [Institution], Speaker; Progenity consultant; Prometheus consultant, Clinical Research [Institution]; Protagonist consultant, DSMB; Receptos consultant, Clinical Research [Institution]; Salix consultant; Samsung Bioepis consultant; Seres Therapeutics consultant, Clinical Research [Institution]; Takeda consultant, Clinical Research [Institution], speaker; UCB consultant, Clinical Research [Institution]; Ventyx DSMB VHsquared consultant. No other authors have any relevant conflicts of interest.
Similar articles
-
Corticosteroid-Free Remission vs Overall Remission in Clinical Trials of Moderate-Severe Ulcerative Colitis and Crohn's Disease.Inflamm Bowel Dis. 2020 Mar 4;26(4):515-523. doi: 10.1093/ibd/izz193. Inflamm Bowel Dis. 2020. PMID: 31504528 Free PMC article.
-
Long-Term Benefit of Mesalamine Granules for Patients Who Achieved Corticosteroid-Induced Ulcerative Colitis Remission.Dig Dis Sci. 2016 Jan;61(1):221-9. doi: 10.1007/s10620-015-3866-7. Epub 2015 Nov 12. Dig Dis Sci. 2016. PMID: 26563167 Free PMC article.
-
Effects of prednisolone tapering on effectiveness of infliximab in patients with ulcerative colitis: data from a retrospective cohort.BMJ Open Gastroenterol. 2024 May 7;11(1):e001343. doi: 10.1136/bmjgast-2024-001343. BMJ Open Gastroenterol. 2024. PMID: 38719549 Free PMC article.
-
Methotrexate Is Not Superior to Placebo for Inducing Steroid-Free Remission, but Induces Steroid-Free Clinical Remission in a Larger Proportion of Patients With Ulcerative Colitis.Gastroenterology. 2016 Feb;150(2):380-8.e4. doi: 10.1053/j.gastro.2015.10.050. Epub 2015 Nov 26. Gastroenterology. 2016. PMID: 26632520 Clinical Trial.
-
Corticosteroid Use in Randomized Clinical Trials of Biologics and Small Molecules in Inflammatory Bowel Disease: A Systematic Review.Inflamm Bowel Dis. 2025 May 12;31(5):1430-1440. doi: 10.1093/ibd/izae240. Inflamm Bowel Dis. 2025. PMID: 39419764
Cited by
-
Acute Severe Ulcerative Colitis: An International Delphi Consensus on Clinical Trial Design and Endpoints.Clin Gastroenterol Hepatol. 2025 Jul;23(8):1408-1417.e4. doi: 10.1016/j.cgh.2024.10.029. Epub 2024 Dec 15. Clin Gastroenterol Hepatol. 2025. PMID: 39681225 Free PMC article.
-
Explainable artificial intelligence for prediction of refractory ulcerative colitis: analysis of a Japanese Nationwide Registry.Ann Med. 2025 Dec;57(1):2499960. doi: 10.1080/07853890.2025.2499960. Epub 2025 May 5. Ann Med. 2025. PMID: 40323686 Free PMC article.
-
Clinical Trial Design Considerations for Hospitalised Patients With Ulcerative Colitis Flares and Application to Study Hyperbaric Oxygen Therapy in the NIDDK HBOT-UC Consortium.Aliment Pharmacol Ther. 2024 Dec;60(11-12):1512-1524. doi: 10.1111/apt.18326. Epub 2024 Oct 15. Aliment Pharmacol Ther. 2024. PMID: 39403018 Free PMC article. Review.
References
-
- Rutgeerts P, Sandborn WJ, Feagan BG, et al.. Infliximab for induction and maintenance therapy for ulcerative colitis. N Engl J Med 2005;353:2462–76. - PubMed
-
- Feagan BG, Rutgeerts P, Sands BE, et al..; GEMINI 1 Study Group. Vedolizumab as induction and maintenance therapy for ulcerative colitis. N Engl J Med 2013;369:699–710. - PubMed
-
- Sandborn WJ, van Assche G, Reinisch W, et al.. Adalimumab induces and maintains clinical remission in patients with moderate-to-severe ulcerative colitis. Gastroenterology 2012;142:257–65.e1. - PubMed
-
- Sandborn WJ, Feagan BG, Marano C, et al..; PURSUIT-Maintenance Study Group. Subcutaneous golimumab maintains clinical response in patients with moderate-to-severe ulcerative colitis. Gastroenterology 2014;146:96–109.e1. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
