

Substitute or coexistence? Mediastinoscopy-assisted versus thoracoscope-assisted esophagectomy in esophageal cancer: a meta-analysis of perioperative outcomes and long-term survival
- PMID: 38869981
- PMCID: PMC11392080
- DOI: 10.1097/JS9.0000000000001777
Substitute or coexistence? Mediastinoscopy-assisted versus thoracoscope-assisted esophagectomy in esophageal cancer: a meta-analysis of perioperative outcomes and long-term survival
Abstract
Background: Currently, mediastinoscopy-assisted esophagectomy (MAE) and thoracoscope-assisted esophagectomy (TAE) represent two prevalent forms of minimally invasive esophagectomy extensively employed in the management of esophageal cancer (EC). The aim of this meta-analysis is to assess and compare these two surgical approaches concerning perioperative outcomes and long-term survival, offering valuable insights for refining surgical strategies and enhancing patient outcomes in this field.
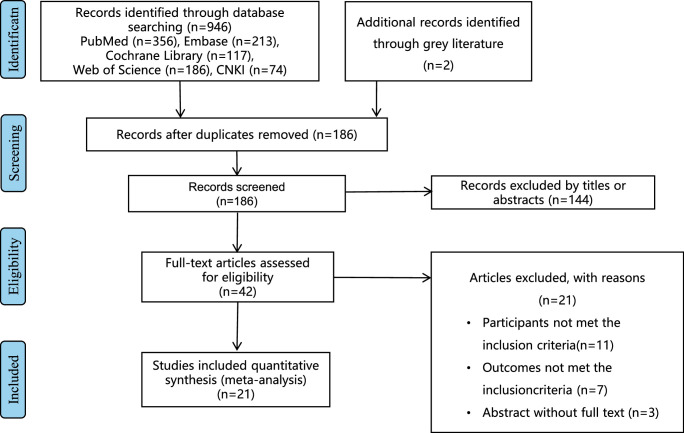
Methods: Adhering to PRISMA guidelines, the authors systematically searched PubMed, Web of Science, Cochrane Library, Embase, and CNKI databases until 1 March 2024, for studies comparing MAE and TAE. Outcomes of interest included perioperative outcomes (intraoperative outcomes, postoperative recovery, postoperative complications) and survival rates. Statistical analyses were performed using RevMan 5.4, with heterogeneity dictating the use of fixed or random-effects models.
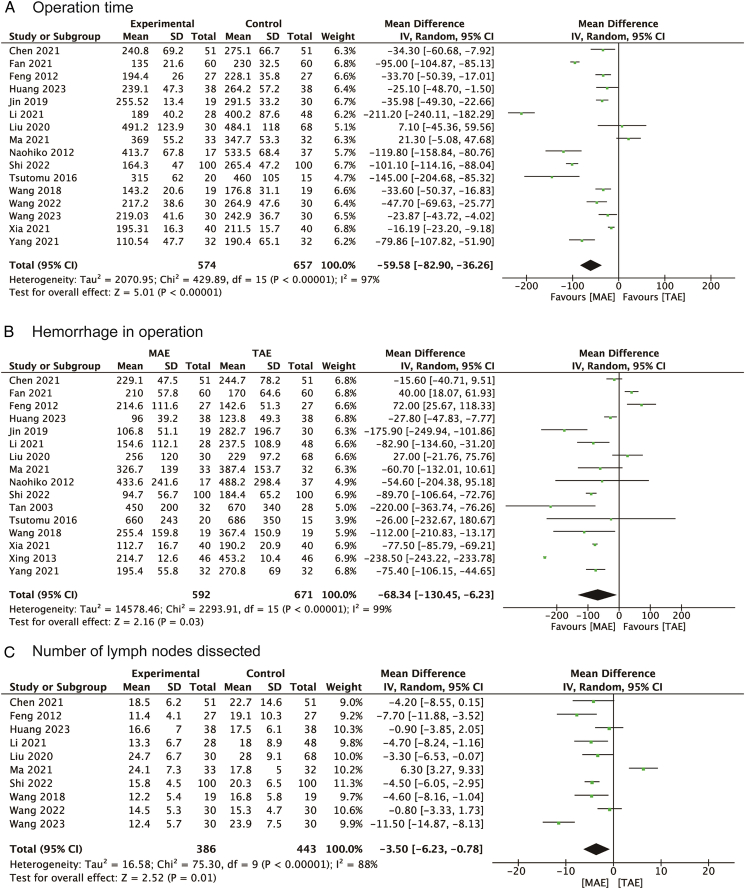
Results: A total of 21 relevant studies were finally included. MAE was associated with significantly shorter operation times [mean difference (MD)=-59.58 min, 95% CI: -82.90 to -36.26] and less intraoperative blood loss (MD=-68.34 ml, 95% CI: -130.45 to -6.23). However, MAE resulted in fewer lymph nodes being dissected (MD=-3.50, 95% CI: -6.23 to -0.78). Postoperative recovery was enhanced following MAE, as evidenced by reduced hospital stays and tube times. MAE significantly reduced pulmonary complications [odds ratio (OR)=0.59, 95% CI: 0.44, 0.81] but increased the incidence of recurrent laryngeal nerve injury (OR=1.84, 95% CI: 1.30, 2.60). No significant differences were observed in anastomotic leakage, chylothorax, cardiac complications, wound infections, and gastric retention between MAE and TAE. The long-term survival outcomes showed no statistical difference [hazard ratio (HR)=1.05, 95% CI: 0.71, 1.54].
Conclusions: MAE offers advantages in reducing operation time, blood loss, and specific postoperative complications, particularly pulmonary complications, with a shorter recovery period compared to TAE. However, it poses a higher risk of recurrent laryngeal nerve injury and results in fewer lymph nodes being dissected. No difference in long-term survival was observed, indicating that both techniques have distinct benefits and limitations. These findings underscore the need for personalized surgical approaches in EC treatment, considering individual patient characteristics and tumor specifics.
Copyright © 2024 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures











Similar articles
-
Comparison of mediastinoscopy and thoracoscope minimally invasive esophagectomy in the treatment of esophageal cancer: a meta-analysis and system review.BMC Cancer. 2025 Jan 6;25(1):14. doi: 10.1186/s12885-024-13307-1. BMC Cancer. 2025. PMID: 39762788 Free PMC article.
-
Safety and Feasibility of Mediastinoscopy-assisted Esophagectomy: A Meta-analysis.Surg Laparosc Endosc Percutan Tech. 2023 Aug 1;33(4):420-427. doi: 10.1097/SLE.0000000000001182. Surg Laparosc Endosc Percutan Tech. 2023. PMID: 37505923
-
Retrospective Comparison of Two Minimally Invasive Esophagectomy in the Treatment of Esophageal Cancer: Pneumatic Mediastinoscopy Versus Thoracoscopy.J Laparoendosc Adv Surg Tech A. 2019 May;29(5):638-642. doi: 10.1089/lap.2018.0512. Epub 2018 Dec 18. J Laparoendosc Adv Surg Tech A. 2019. PMID: 30562122
-
Comparison of Clinical Outcomes of Robot-Assisted, Video-Assisted, and Open Esophagectomy for Esophageal Cancer: A Systematic Review and Meta-analysis.JAMA Netw Open. 2021 Nov 1;4(11):e2129228. doi: 10.1001/jamanetworkopen.2021.29228. JAMA Netw Open. 2021. PMID: 34724556 Free PMC article.
-
Short-term outcomes of robot-assisted versus conventional minimally invasive esophagectomy for esophageal cancer: a systematic review and meta-analysis of 18,187 patients.J Robot Surg. 2024 Mar 16;18(1):125. doi: 10.1007/s11701-024-01880-3. J Robot Surg. 2024. PMID: 38492067 Free PMC article.
Cited by
-
Comparison of mediastinoscopy and thoracoscope minimally invasive esophagectomy in the treatment of esophageal cancer: a meta-analysis and system review.BMC Cancer. 2025 Jan 6;25(1):14. doi: 10.1186/s12885-024-13307-1. BMC Cancer. 2025. PMID: 39762788 Free PMC article.
-
Efficacy of Dexmedetomidine as an Adjuvant to Ropivacaine for Intercostal Nerve Block in Elderly Patients Undergoing Video-Assisted Thoracoscopic Esophagectomy: A randomized Double-Blinded Trial.J Pain Res. 2025 Aug 12;18:4019-4027. doi: 10.2147/JPR.S542327. eCollection 2025. J Pain Res. 2025. PMID: 40822432 Free PMC article. Clinical Trial.
-
Effects of the lavage through fistula in treatment of spontaneous esophageal rupture by combined thoracoscopic and gastroscopic management.World J Emerg Surg. 2025 Jun 7;20(1):51. doi: 10.1186/s13017-025-00630-6. World J Emerg Surg. 2025. PMID: 40483493 Free PMC article.
-
Mediastinoscopy-Assisted Esophagectomy as an Effective Treatment for IgG4-Related Esophageal Stenosis: A Case Report.Surg Case Rep. 2025;11(1):25-0346. doi: 10.70352/scrj.cr.25-0346. Epub 2025 Jul 29. Surg Case Rep. 2025. PMID: 40746982 Free PMC article.
References
-
- Sung H, Ferlay J, Siegel RL, et al. . Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2021;71:209–249. - PubMed
-
- Lagergren J, Smyth E, Cunningham D, et al. . Oesophageal cancer. Lancet 2017;390:2383–2396. - PubMed
-
- Kelly RJ. Emerging multimodality approaches to treat localized esophageal cancer. J Natl Compr Canc Netw 2019;17:1009–1014. - PubMed
-
- Jin Y, Lu X, Xue L, et al. . Retrospective comparison of two minimally invasive esophagectomy in the treatment of esophageal cancer: pneumatic mediastinoscopy versus thoracoscopy. J Laparoendosc Adv Surg Tech A 2019;29:638–642. - PubMed
-
- Gottlieb-Vedi E, Kauppila JH, Malietzis G, et al. . Long-term survival in esophageal cancer after minimally invasive compared to open esophagectomy: a systematic review and meta-analysis. Ann Surg 2019;270:1005–1017. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
