

Statins, metformin, and RAS inhibitors did not reduce variceal bleeding risk and mortality in a large, real-life cohort of patients with cirrhosis
- PMID: 38870117
- PMCID: PMC11175511
- DOI: 10.1371/journal.pone.0302811
Statins, metformin, and RAS inhibitors did not reduce variceal bleeding risk and mortality in a large, real-life cohort of patients with cirrhosis
Abstract
Background: Previous experimental and clinical studies suggested a beneficial effect of statins, metformin, angiotensin-converting-enzyme inhibitors and angiotensin II receptor blockers (RASi) on portal hypertension. Still, their effects on hard cirrhosis-related clinical endpoints, such as variceal bleeding and bleeding-related mortality, remain to be investigated.
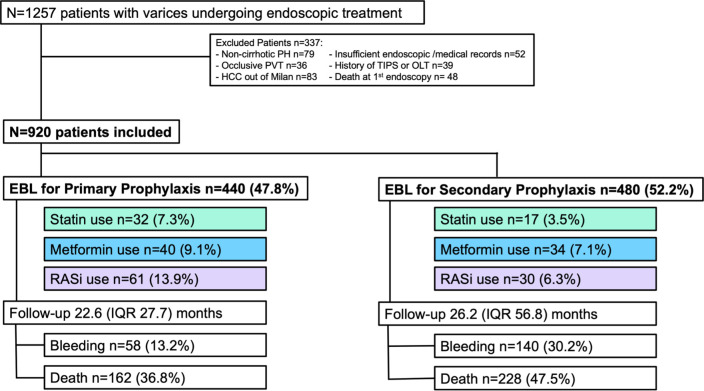
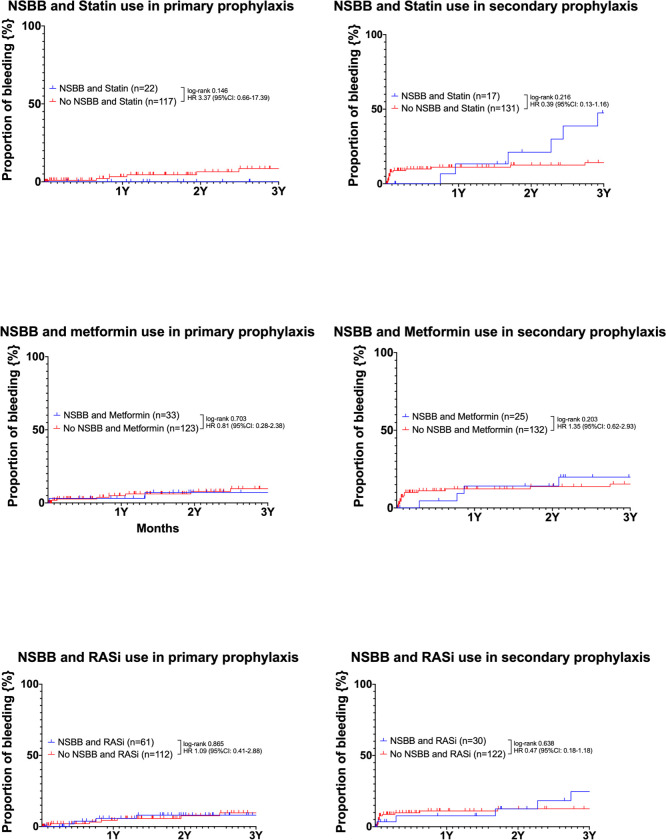
Methods: Thus, we recorded the use of statins, metformin and RASi in a large cohort of cirrhotic patients undergoing endoscopic band ligation (EBL) for primary (PP, n = 440) and secondary bleeding prophylaxis (SP, n = 480) between 01/2000 and 05/2020. Variceal (re-) bleeding and survival rates were compared between patients with vs. without these co-medications.
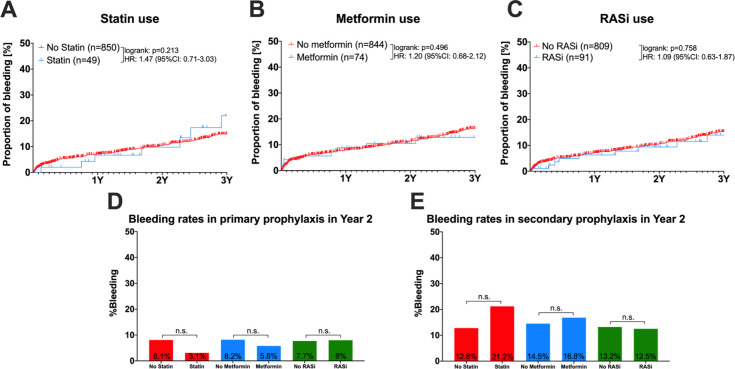
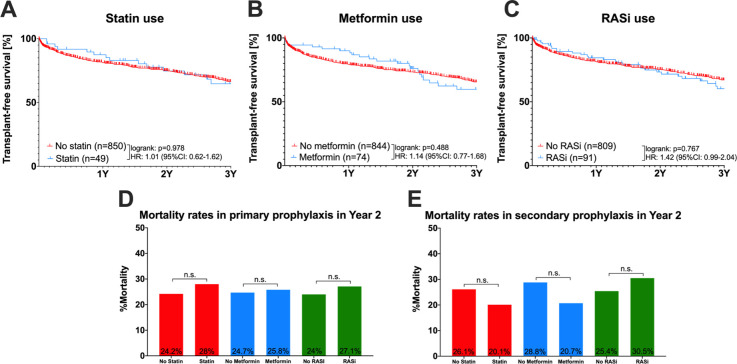
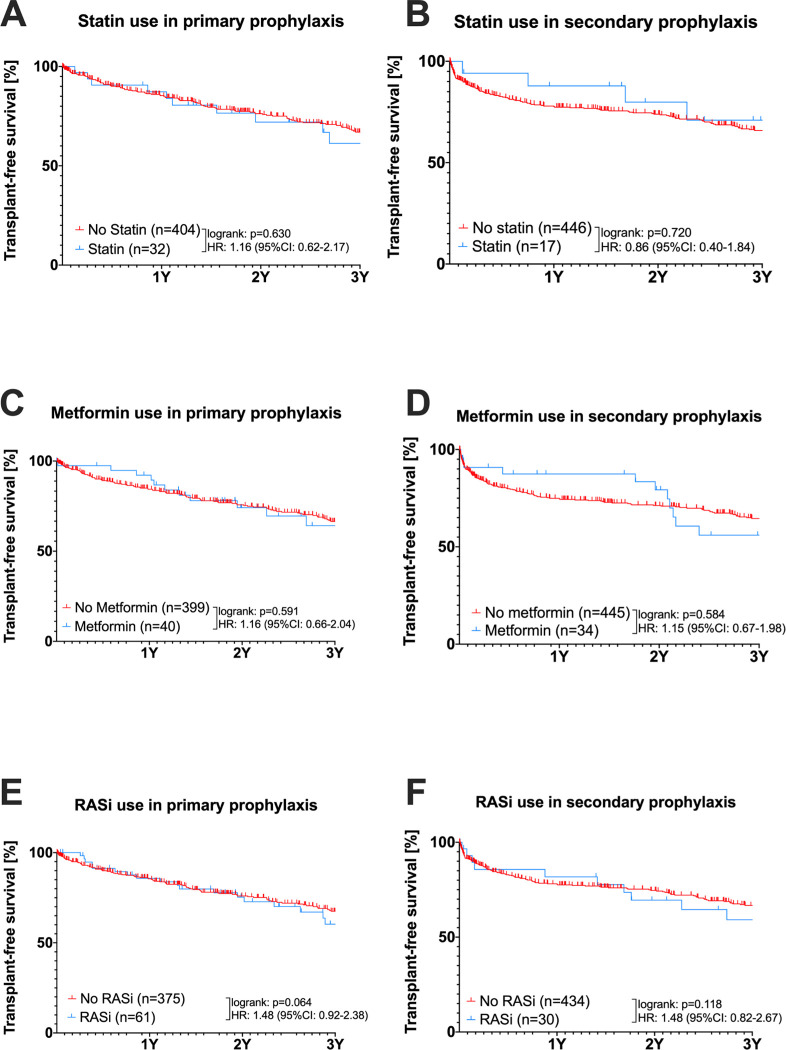
Results: A total of 920 cirrhotic patients with varices were included. At first EBL, median MELD was 13 and 515 (56%) patients showed ascites. Statins, metformin and RASi were used by 49 (5.3%), 74 (8%), and 91 (9.9%) patients, respectively. MELD and platelet counts were similar in patients with and without the co-medications of interest. Rates of first variceal bleeding and variceal rebleeding at 2 years were 5.2% and 11.7%, respectively. Neither of the co-medications were associated with decreased first bleeding rates (log-rank tests in PP: statins p = 0.813, metformin p = 0.862, RASi p = 0.919) nor rebleeding rates (log-rank tests in SP: statin p = 0.113, metformin p = 0.348, RASi p = 0.273). Similar mortality rates were documented in patients with and without co-medications for PP (log-rank tests: statins p = 0.630, metformin p = 0.591, RASi p = 0.064) and for SP (statins p = 0.720, metformin p = 0.584, RASi p = 0.118).
Conclusion: In clinical practice, variceal bleeding and mortality rates of cirrhotic patients were not reduced by co-medication with statins, metformin or RASi. Nevertheless, we recommend the use of these co-medications by indication, as they may still exert beneficial effects on non-bleeding complications in patients with liver cirrhosis.
Copyright: © 2024 Pfisterer et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Betablockers do not increase efficacy of band ligation in primary prophylaxis but they improve survival in secondary prophylaxis of variceal bleeding.Aliment Pharmacol Ther. 2018 Apr;47(7):966-979. doi: 10.1111/apt.14485. Epub 2018 Feb 1. Aliment Pharmacol Ther. 2018. PMID: 29388229
-
Addition of Simvastatin to Standard Therapy for the Prevention of Variceal Rebleeding Does Not Reduce Rebleeding but Increases Survival in Patients With Cirrhosis.Gastroenterology. 2016 May;150(5):1160-1170.e3. doi: 10.1053/j.gastro.2016.01.004. Epub 2016 Jan 14. Gastroenterology. 2016. PMID: 26774179 Clinical Trial.
-
Pharmacologic prevention of variceal bleeding and rebleeding.Hepatol Int. 2018 Feb;12(Suppl 1):68-80. doi: 10.1007/s12072-017-9833-y. Epub 2017 Dec 5. Hepatol Int. 2018. PMID: 29210030 Review.
-
Current and future pharmacological therapies for managing cirrhosis and its complications.World J Gastroenterol. 2019 Feb 28;25(8):888-908. doi: 10.3748/wjg.v25.i8.888. World J Gastroenterol. 2019. PMID: 30833797 Free PMC article. Review.
-
Covered TIPS versus endoscopic band ligation plus propranolol for the prevention of variceal rebleeding in cirrhotic patients with portal vein thrombosis: a randomised controlled trial.Gut. 2018 Dec;67(12):2156-2168. doi: 10.1136/gutjnl-2017-314634. Epub 2017 Sep 28. Gut. 2018. PMID: 28970291 Clinical Trial.
Cited by
-
The CYP4/20-HETE/GPR75 axis in the progression metabolic dysfunction-associated steatosis liver disease (MASLD) to chronic liver disease.Front Physiol. 2025 Jan 29;15:1497297. doi: 10.3389/fphys.2024.1497297. eCollection 2024. Front Physiol. 2025. PMID: 39959811 Free PMC article.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
