

Early-stage health technology assessment of fractional flow reserve coronary computed tomography versus standard diagnostics in patients with stable chest pain in The Netherlands
- PMID: 38870138
- PMCID: PMC11175410
- DOI: 10.1371/journal.pone.0305189
Early-stage health technology assessment of fractional flow reserve coronary computed tomography versus standard diagnostics in patients with stable chest pain in The Netherlands
Abstract
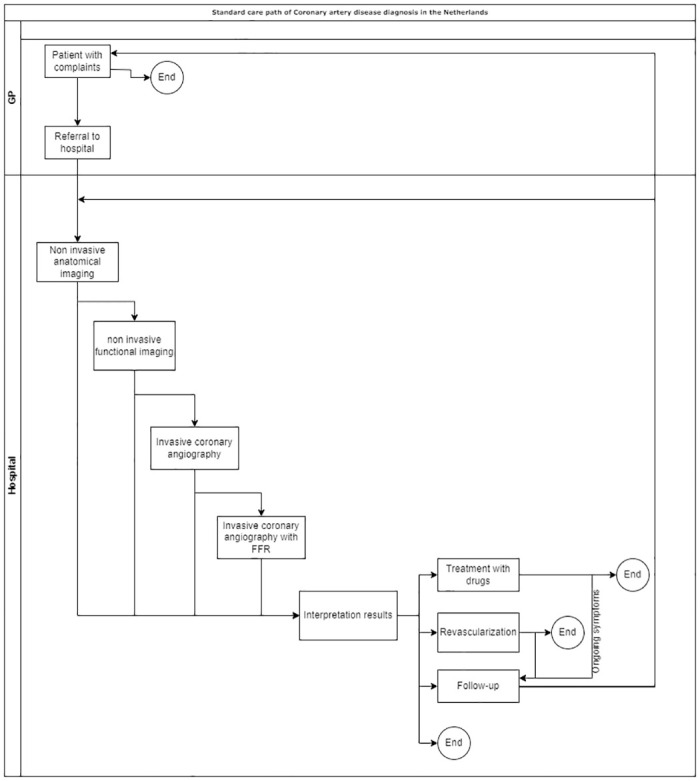
Objectives: The aim of this early-stage Health Technology Assessment (HTA) was to assess the difference in healthcare costs and effects of fractional flow reserve derived from coronary computed tomography (FFRct) compared to standard diagnostics in patients with stable chest pain in The Netherlands.
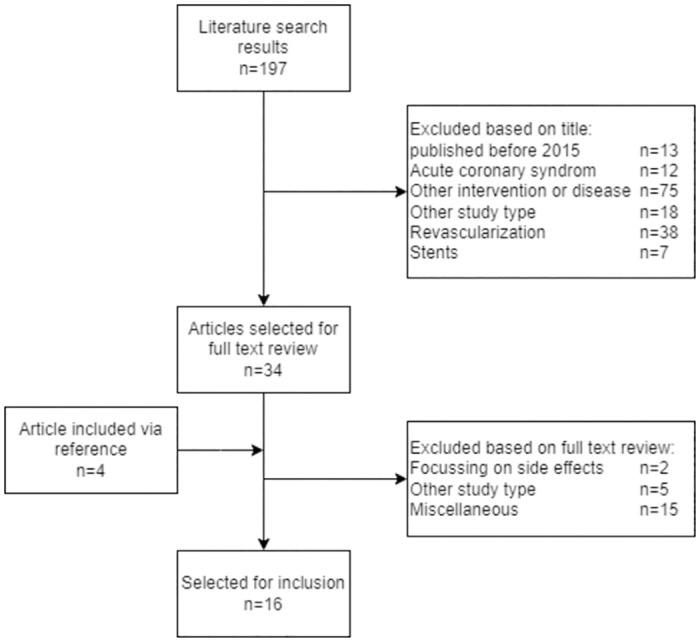
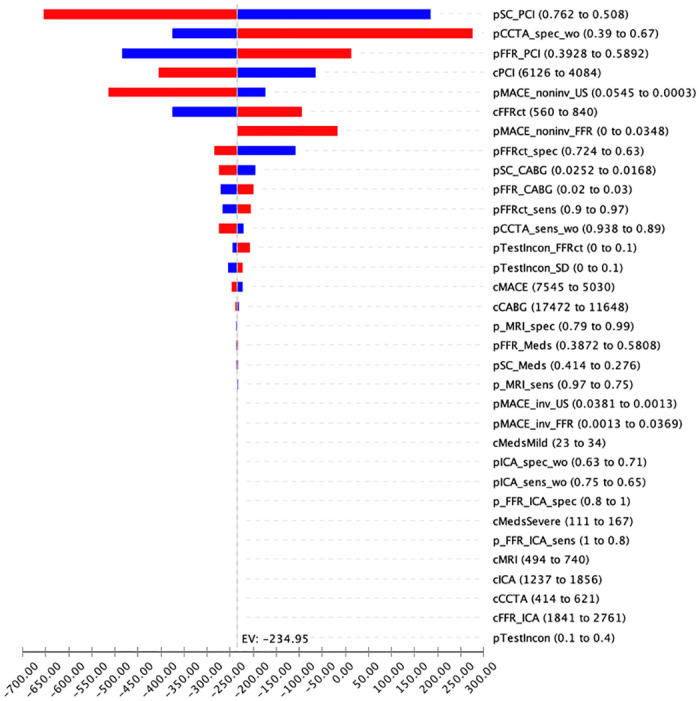
Methods: A decision-tree model was developed to assess the difference in total costs from the hospital perspective, probability of correct diagnoses, and risk of major adverse cardiovascular events at one year follow-up. One-way sensitivity analyses were conducted to determine the main drivers of the cost difference between the strategies. A threshold analysis on the added price of FFRct analysis (computational analysis only) was conducted.
Results: The mean one-year costs were €2,680 per patient for FFRct and €2,915 per patient for standard diagnostics. The one-year probability of correct diagnoses was 0.78 and 0.61, and the probability of major adverse cardiovascular events was 1.92x10-5 and 0.01, respectively. The probability and costs of revascularization and the specificity of coronary computed tomography angiography had the greatest effect on the difference in costs between the strategies. The added price of FFRct analysis should be below €935 per patient to be considered the least costly option.
Conclusions: The early-stage HTA findings suggest that FFRct may reduce total healthcare spending, probability of incorrect diagnoses, and major adverse cardiovascular events compared to current diagnostics for patients with stable chest pain in the Dutch healthcare setting over one year. Future cost-effectiveness studies should determine a value-based pricing for FFRct and quantify the economic value of the anticipated therapeutic impact.
Copyright: © 2024 Boot et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Cost-effectiveness Analysis of Anatomic vs Functional Index Testing in Patients With Low-Risk Stable Chest Pain.JAMA Netw Open. 2020 Dec 1;3(12):e2028312. doi: 10.1001/jamanetworkopen.2020.28312. JAMA Netw Open. 2020. PMID: 33315111 Free PMC article. Clinical Trial.
-
Quality-of-Life and Economic Outcomes of Assessing Fractional Flow Reserve With Computed Tomography Angiography: PLATFORM.J Am Coll Cardiol. 2015 Dec 1;66(21):2315-2323. doi: 10.1016/j.jacc.2015.09.051. Epub 2015 Oct 14. J Am Coll Cardiol. 2015. PMID: 26475205 Clinical Trial.
-
Comparative efficacy testing - fractional flow reserve by coronary computed tomography for the evaluation of patients with stable chest pain.Int J Cardiol. 2015 Mar 15;183:173-7. doi: 10.1016/j.ijcard.2015.01.035. Epub 2015 Jan 27. Int J Cardiol. 2015. PMID: 25666127
-
Utility of FFRCT in Patients with Chest Pain.Curr Atheroscler Rep. 2023 Aug;25(8):427-434. doi: 10.1007/s11883-023-01117-y. Epub 2023 Jun 26. Curr Atheroscler Rep. 2023. PMID: 37358803 Review.
-
Computed tomography angiography-derived fractional flow reserve (CT-FFR) for the detection of myocardial ischemia with invasive fractional flow reserve as reference: systematic review and meta-analysis.Eur Radiol. 2020 Feb;30(2):712-725. doi: 10.1007/s00330-019-06470-8. Epub 2019 Nov 6. Eur Radiol. 2020. PMID: 31696294
References
-
- Environment NIfPHat. Rankings of conditions based on mortality in 2020 [March 22, 2023]. https://vzinfo.nl/ranglijsten/sterfte.
-
- Environment NIfPHat. Ranking of conditions based on burden of disease in DALY’s 2018 [March 22, 2023]. https://www.vzinfo.nl/ranglijsten/aandoeningen-op-basis-van-ziektelast
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
