

A rare intraosseous synovial sarcoma of the mandible: A case report
- PMID: 38870657
- PMCID: PMC11225348
- DOI: 10.1016/j.ijscr.2024.109880
A rare intraosseous synovial sarcoma of the mandible: A case report
Abstract
Introduction: Synovial sarcoma is a relatively common high-grade soft-tissue sarcoma. This lesion accounts for 5-10 % of soft-tissue sarcomas, which tend to appear in the limbs, especially the lower limbs. Synovial sarcoma in the neck is rare and causes involvement of the head and neck in 6-7 % of cases. Intraosseous involvement of the mandible is rare. In this report, a rare intraosseous synovial sarcoma of the mandible is reported.
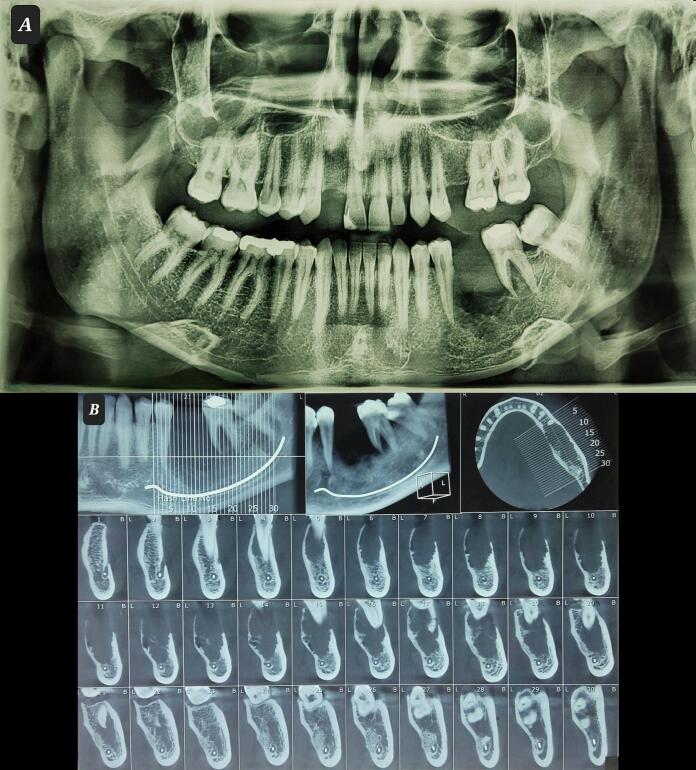
Presentation of case: A 29-year-old man with a complaint of painless outgrowth of the gingiva in the posterior region of the left mandible. In the intraoral examination, an exophytic, firm, smooth and well-defined lobulated mass on the alveolar ridge, extending from distal of the second premolar to mesial of the second molar, was observed. On a radiographic examination, a radiolucent lesion with an ill-defined border was seen in the left body of the mandibular with perforation of the buccal cortex. In a histological examination, immunohistochemistry confirmed synovial sarcoma. The patient underwent surgery with wide margins, and radiotherapy after surgery.
Discussion: The main treatment method is surgery with a wide margin. Radiotherapy as an adjuvant treatment along with surgery is the second most common treatment method. Radiotherapy is recommended in cases of involvement of the margin of the lesion, size greater than 5 cm, and recurrence of the lesion. Chemotherapy after surgery has been used less frequently.
Conclusion: Surgical resection with a wide margin is the main treatment. Adjuvant radiation therapy and chemotherapy can be helpful in tumor control, especially in monophasic cases.
Keywords: Head and neck sarcoma; Immunohistochemistry; Intraosseous; Synovial sarcoma.
Copyright © 2024 The Authors. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Conflict of interest statement None declared. The authors have no financial, consultative, institutional, and other relationships that might lead to bias or conflict of interest.
Figures




Similar articles
-
Inguinal synovial sarcoma revealed by a limb swelling: A case report.Int J Surg Case Rep. 2024 Feb;115:109252. doi: 10.1016/j.ijscr.2024.109252. Epub 2024 Jan 12. Int J Surg Case Rep. 2024. PMID: 38241792 Free PMC article.
-
Primary pancreatic synovial sarcoma: Report of a rare case and review of the literature.Med Int (Lond). 2023 Mar 24;3(3):22. doi: 10.3892/mi.2023.82. eCollection 2023 May-Jun. Med Int (Lond). 2023. PMID: 37214230 Free PMC article.
-
Primary Intraosseous Synovial Sarcoma with Molecular Confirmation: Expanding and Clarifying the Spectrum of This Rare Neoplasm.Case Rep Pathol. 2020 Jan 28;2020:5492754. doi: 10.1155/2020/5492754. eCollection 2020. Case Rep Pathol. 2020. PMID: 32082672 Free PMC article.
-
Monophasic synovial sarcoma arising in the vulva: a case report and review of the literature.Arch Pathol Lab Med. 2008 Apr;132(4):698-702. doi: 10.5858/2008-132-698-MSSAIT. Arch Pathol Lab Med. 2008. PMID: 18384223 Review.
-
Intracranial primary synovial sarcoma mimicking a spontaneous cerebral hematoma-a case report and review of the literature.Neurochirurgie. 2022 Jul;68(4):443-446. doi: 10.1016/j.neuchi.2021.08.003. Epub 2021 Aug 31. Neurochirurgie. 2022. PMID: 34478758 Review.
Cited by
-
Intraoral Immature Malignant Teratoma with No Evidence of Other Sites of Involvement in a 6-Year-Old Patient: A Case Report.Reports (MDPI). 2024 Dec 27;8(1):3. doi: 10.3390/reports8010003. Reports (MDPI). 2024. PMID: 40729216 Free PMC article.
References
-
- Donohoe E., et al. Molecular confirmation of primary monophasic synovial sarcoma of the mandible: diagnosis and management. Br. J. Oral Maxillofac. Surg. 2022;60(7):994–996. - PubMed
-
- Liu Z., et al. Management of the primary intraosseous synovial sarcoma of the jaws: be careful of the surgical margin. J. Oral Maxillofac. Surg. 2015;73(3):550–563. - PubMed
-
- Stanbouly D., et al. Synovial sarcoma of the head & neck: a review of reported cases in the literature. Journal of Stomatology, Oral and Maxillofacial Surgery. 2021;122(5):505–510. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
