

A Case of Severe Delayed Vasospasm after Clipping Surgery for an Unruptured Intracranial Aneurysm
- PMID: 38871004
- PMCID: PMC11222685
- DOI: 10.5469/neuroint.2024.00150
A Case of Severe Delayed Vasospasm after Clipping Surgery for an Unruptured Intracranial Aneurysm
Abstract
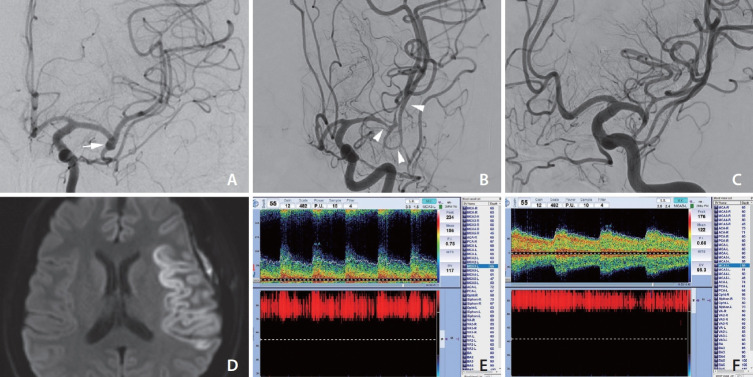
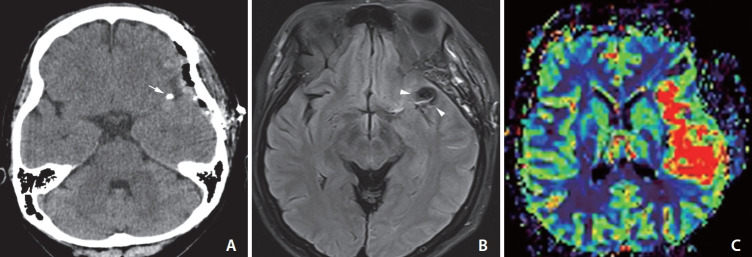
Delayed ischemic stroke associated with intractable vasospasm after clipping of unruptured intracranial aneurysms (UIAs) has been rarely reported. We report a patient with delayed ischemic stroke associated with intractable vasospasm following UIA clipping. A middle-aged female underwent surgery for unruptured middle cerebral artery bifurcation aneurysms. The patient tolerated the neurosurgical procedure well. Seven days postoperatively, the headache was unbearable; a postcraniotomy headache persisted and abruptly presented with global aphasia and right-sided hemiplegia after a nap. Emergency digital subtraction angiography showed severe luminal narrowing with segmental vasoconstriction, consistent with severe vasospasm. The patient's neurological deficit improved after chemical angioplasty. Neurosurgeons should pay close attention to this treatable/preventive entity after neurological deterioration following UIA clipping, even in patients without subarachnoid hemorrhage.
Keywords: Aneurysm; Angioplasty; Headache; Ischemic stroke.
Conflict of interest statement
YS has been the assistant editor of
Figures
Similar articles
-
Vasospasm and delayed cerebral ischemia after uneventful clipping of an unruptured intracranial aneurysm - a case report.BMC Neurol. 2019 Sep 16;19(1):226. doi: 10.1186/s12883-019-1458-4. BMC Neurol. 2019. PMID: 31526396 Free PMC article.
-
Recurrent Cerebral Vasospasm and Delayed Cerebral Ischemia Weeks Subsequent to Elective Clipping of an Unruptured Middle Cerebral Artery Aneurysm.World Neurosurg. 2020 Sep;141:52-58. doi: 10.1016/j.wneu.2020.05.235. Epub 2020 May 31. World Neurosurg. 2020. PMID: 32492543
-
Unruptured aneurysmal clipping complicated by delayed and refractory vasospasm: case report.BMC Neurol. 2020 Sep 12;20(1):344. doi: 10.1186/s12883-020-01925-8. BMC Neurol. 2020. PMID: 32919459 Free PMC article.
-
Cerebral vasospasm and delayed ischaemic deficit following elective aneurysm clipping.J Clin Neurosci. 2016 Dec;34:33-38. doi: 10.1016/j.jocn.2016.06.006. Epub 2016 Sep 3. J Clin Neurosci. 2016. PMID: 27597383 Review.
-
Comprehensive review of imaging of intracranial aneurysms and angiographically negative subarachnoid hemorrhage.Neurosurg Focus. 2019 Dec 1;47(6):E20. doi: 10.3171/2019.9.FOCUS19653. Neurosurg Focus. 2019. PMID: 31786554 Review.
Cited by
-
Combined microscopic and neuroendoscopic treatment effects on psychological and cognitive outcomes in ruptured intracranial aneurysms.World J Psychiatry. 2025 Mar 19;15(3):100565. doi: 10.5498/wjp.v15.i3.100565. eCollection 2025 Mar 19. World J Psychiatry. 2025. PMID: 40109993 Free PMC article.
References
-
- Vlak MH, Algra A, Brandenburg R, Rinkel GJ. Prevalence of unruptured intracranial aneurysms, with emphasis on sex, age, comorbidity, country, and time period: a systematic review and meta-analysis. Lancet Neurol. 2011;10:626–636. - PubMed
-
- Fu AY, Kumarapuram S, Sreenivasan S, Roychowdhury S, Gupta G. Trends in global research for treating intracranial aneurysms: a bibliometric analysis. World Neurosurg. 2023;177:143–151.e4. - PubMed
-
- Scullen T, Mathkour M, Nerva JD, Dumont AS, Amenta PS. Editorial. Clipping versus coiling for the treatment of middle cerebral artery aneurysms: which modality should be considered first? J Neurosurg. 2019;133:1120–1123. - PubMed
-
- Pflaeging M, Kabbasch C, Schlamann M, Pennig L, Juenger ST, Grunz JP, et al. Microsurgical clipping versus advanced endovascular treatment of unruptured middle cerebral artery bifurcation aneurysms after a “coil-first” policy. World Neurosurg. 2021;149:e336–e344. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
