

Serum cytokine dysregulation signatures associated with COVID-19 outcomes in high mortality intensive care unit cohorts across pandemic waves and variants
- PMID: 38871772
- PMCID: PMC11176334
- DOI: 10.1038/s41598-024-64384-y
Serum cytokine dysregulation signatures associated with COVID-19 outcomes in high mortality intensive care unit cohorts across pandemic waves and variants
Abstract
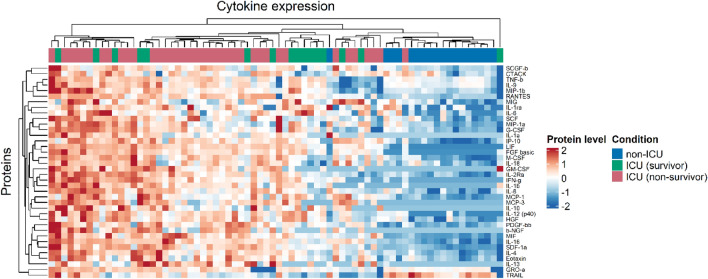
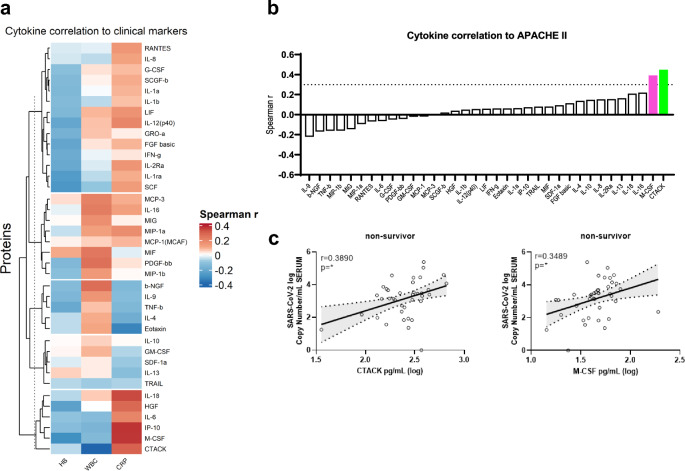
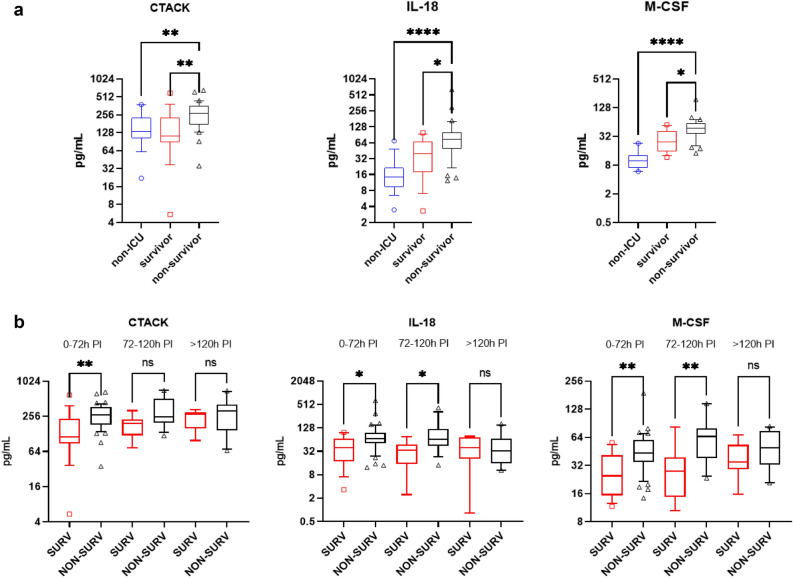
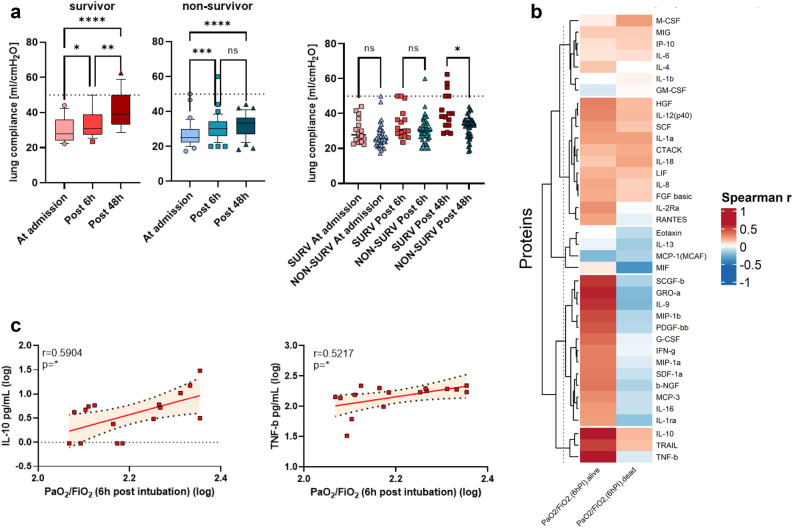
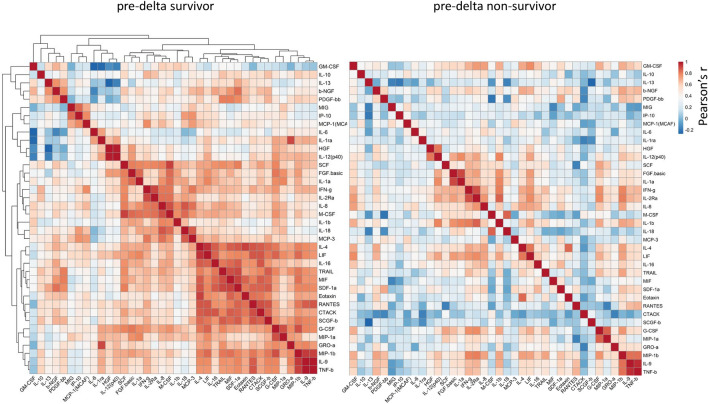
The aim of this study was to characterize the systemic cytokine signature of critically ill COVID-19 patients in a high mortality setting aiming to identify biomarkers of severity, and to explore their associations with viral loads and clinical characteristics. We studied two COVID-19 critically ill patient cohorts from a referral centre located in Central Europe. The cohorts were recruited during the pre-alpha/alpha (November 2020 to April 2021) and delta (end of 2021) period respectively. We determined both the serum and bronchoalveolar SARS-CoV-2 viral load and identified the variant of concern (VoC) involved. Using a cytokine multiplex assay, we quantified systemic cytokine concentrations and analyzed their relationship with clinical findings, routine laboratory workup and pulmonary function data obtained during the ICU stay. Patients who did not survive had a significantly higher systemic and pulmonary viral load. Patients infected with the pre-alpha VoC showed a significantly lower viral load in comparison to those infected with the alpha- and delta-variants. Levels of systemic CTACK, M-CSF and IL-18 were significantly higher in non-survivors in comparison to survivors. CTACK correlated directly with APACHE II scores. We observed differences in lung compliance and the association between cytokine levels and pulmonary function, dependent on the VoC identified. An intra-cytokine analysis revealed a loss of correlation in the non-survival group in comparison to survivors in both cohorts. Critically ill COVID-19 patients exhibited a distinct systemic cytokine profile based on their survival outcomes. CTACK, M-CSF and IL-18 were identified as mortality-associated analytes independently of the VoC involved. The Intra-cytokine correlation analysis suggested the potential role of a dysregulated systemic network of inflammatory mediators in severe COVID-19 mortality.
Keywords: Biomarker; COVID-19; Cytokines; Mortality; SARS-CoV-2; Variant of concern.
© 2024. The Author(s).
Conflict of interest statement
LCS received consulting fees by CORAT Therapeutics, DIGID Diagnostics, Dr. Wolff Group and SANOFI Pharma. LCS received speaker’s honoraria by SWIXX Pharma and SANOFI Pharma. LCS has the following patents: EP3655526 and EP22153256.7. LCS has unpaid positions in the HZI Board of Trustees, he is a member of the Vaccine task force of the European Federation of Immunological Societies and is the co-coordinator for the Vaccine group of the German Immunological Society. Other authors have no competing interest.
Figures
References
-
- Balnis J, Adam AP, Chopra A, Chieng HC, Drake LA, Martino N, et al. Unique inflammatory profile is associated with higher SARS-CoV-2 acute respiratory distress syndrome (ARDS) mortality. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2021;320(3):R250–R257. doi: 10.1152/ajpregu.00324.2020. - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
