

High-resolution adaptive optics-trans-scleral flood illumination (AO-TFI) imaging of retinal pigment epithelium (RPE) in central serous chorioretinopathy (CSCR)
- PMID: 38871803
- PMCID: PMC11176374
- DOI: 10.1038/s41598-024-64524-4
High-resolution adaptive optics-trans-scleral flood illumination (AO-TFI) imaging of retinal pigment epithelium (RPE) in central serous chorioretinopathy (CSCR)
Abstract
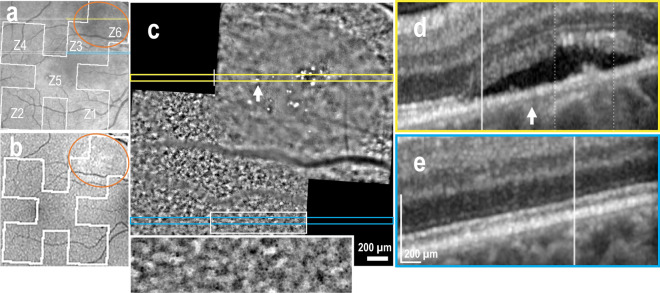
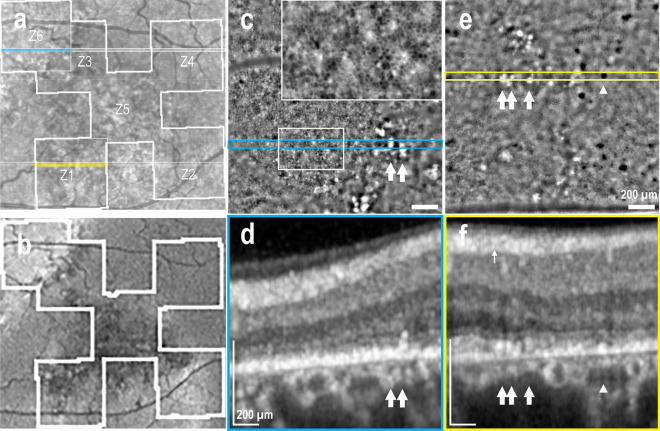
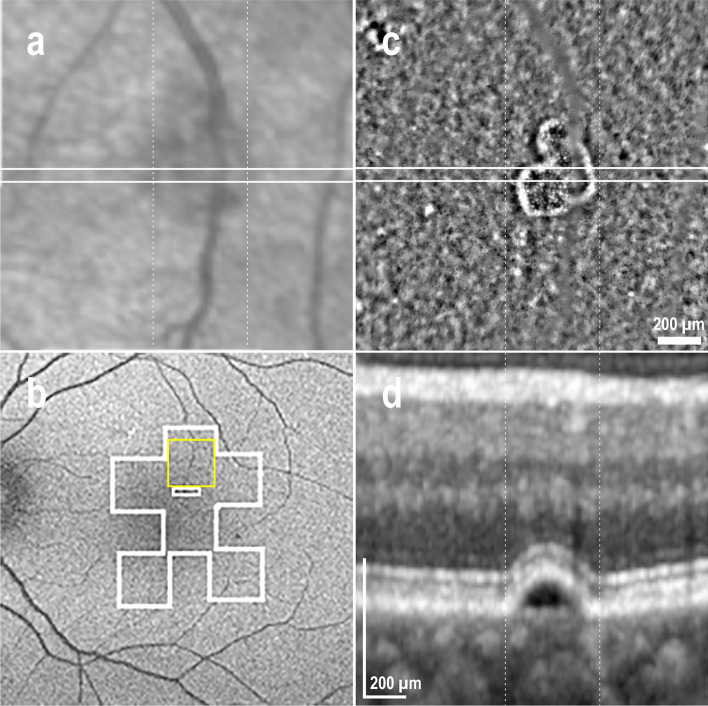
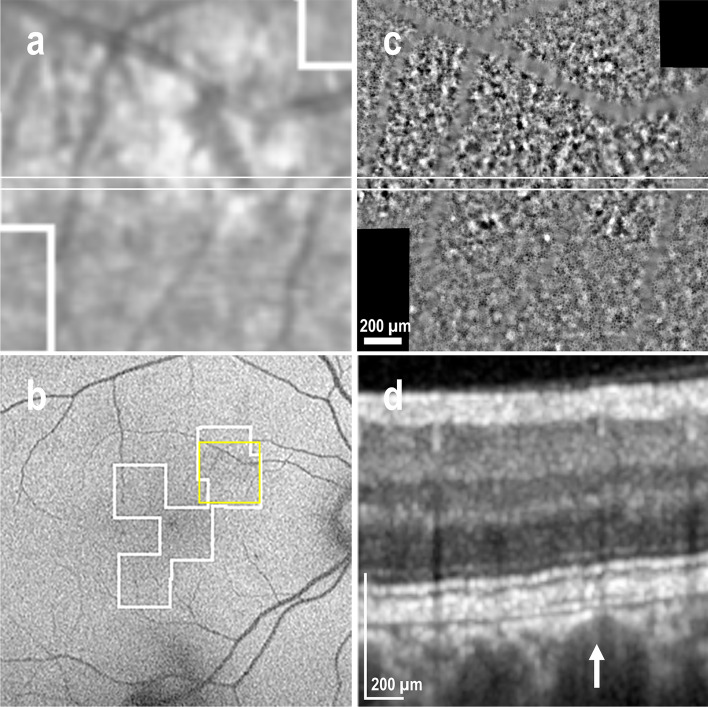
This study aims to correlate adaptive optics-transscleral flood illumination (AO-TFI) images of the retinal pigment epithelium (RPE) in central serous chorioretinopathy (CSCR) with standard clinical images and compare cell morphological features with those of healthy eyes. After stitching 125 AO-TFI images acquired in CSCR eyes (including 6 active CSCR, 15 resolved CSCR, and 3 from healthy contralateral), 24 montages were correlated with blue-autofluorescence, infrared and optical coherence tomography images. All 68 AO-TFI images acquired in pathological areas exhibited significant RPE contrast changes. Among the 52 healthy areas in clinical images, AO-TFI revealed a normal RPE mosaic in 62% of the images and an altered RPE pattern in 38% of the images. Morphological features of the RPE cells were quantified in 54 AO-TFI images depicting clinically normal areas (from 12 CSCR eyes). Comparison with data from 149 AO-TFI images acquired in 33 healthy eyes revealed significantly increased morphological heterogeneity. In CSCR, AO-TFI not only enabled high-resolution imaging of outer retinal alterations, but also revealed RPE abnormalities undetectable by all other imaging modalities. Further studies are required to estimate the prognosis value of these abnormalities. Imaging of the RPE using AO-TFI holds great promise for improving our understanding of the CSCR pathogenesis.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests
Figures




Similar articles
-
Adaptive Optics-Transscleral Flood Illumination Imaging of Retinal Pigment Epithelium in Dry Age-Related Macular Degeneration.Cells. 2025 Apr 24;14(9):633. doi: 10.3390/cells14090633. Cells. 2025. PMID: 40358157 Free PMC article.
-
Retro-mode Imaging for retinal pigment epithelium alterations in central serous chorioretinopathy.Am J Ophthalmol. 2012 Jul;154(1):155-163.e4. doi: 10.1016/j.ajo.2012.01.023. Epub 2012 Apr 13. Am J Ophthalmol. 2012. PMID: 22503695
-
Multicolor imaging in central serous chorioretinopathy - a quantitative and qualitative comparison with fundus autofluorescence.Sci Rep. 2019 Aug 13;9(1):11728. doi: 10.1038/s41598-019-48040-4. Sci Rep. 2019. PMID: 31409843 Free PMC article.
-
[Pathophysiology of macular diseases--morphology and function].Nippon Ganka Gakkai Zasshi. 2011 Mar;115(3):238-74; discussion 275. Nippon Ganka Gakkai Zasshi. 2011. PMID: 21476310 Review. Japanese.
-
Central Serous Chorioretinopathy.Adv Exp Med Biol. 2025;1467:277-280. doi: 10.1007/978-3-031-72230-1_53. Adv Exp Med Biol. 2025. PMID: 40736855 Review.
Cited by
-
Adaptive Optics-Transscleral Flood Illumination Imaging of Retinal Pigment Epithelium in Dry Age-Related Macular Degeneration.Cells. 2025 Apr 24;14(9):633. doi: 10.3390/cells14090633. Cells. 2025. PMID: 40358157 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
