

A case of TAFRO syndrome after vaccination, successfully treated with cyclosporine
- PMID: 38872134
- PMCID: PMC11177486
- DOI: 10.1186/s12882-024-03630-x
A case of TAFRO syndrome after vaccination, successfully treated with cyclosporine
Abstract
Background: TAFRO syndrome is a rare disorder that causes thrombocytopenia, generalized oedema, fever, organ enlargement, and renal impairment. Few reports have suggested an association with vaccines, and few cases have undergone renal biopsy. TAFRO syndrome is often severe and fatal, and its cause is unknown. We report a case of TAFRO syndrome that occurred after vaccination with the coronavirus disease 2019 (COVID-19) vaccine.
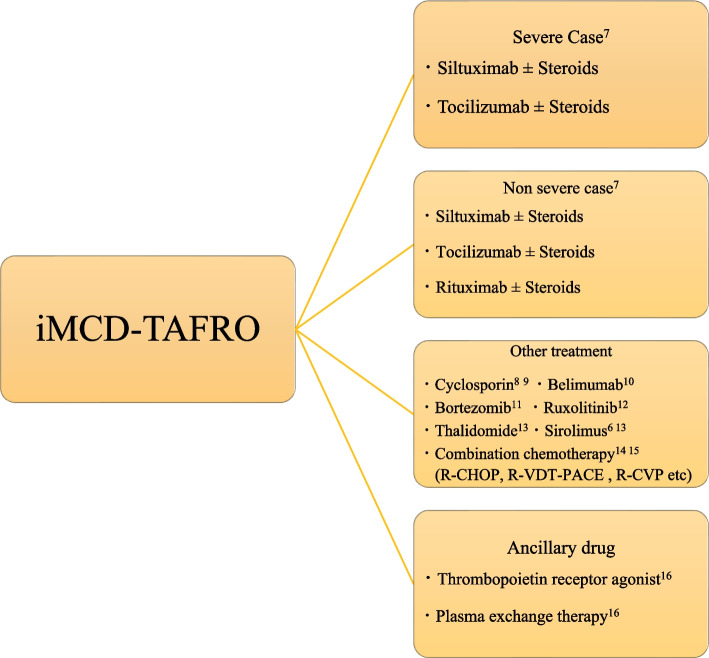
Case presentation: An 82-year-old woman received two doses of the BNT162b2 mRNA vaccine 3 weeks apart. Two weeks later, she was admitted to the hospital with oedema, accompanied with renal failure and thrombocytopenia. After close examination, she was diagnosed with TAFRO syndrome. She was treated with steroids, cyclosporine, and thrombopoietin receptor agonists. The patient was discharged after several months in remission.
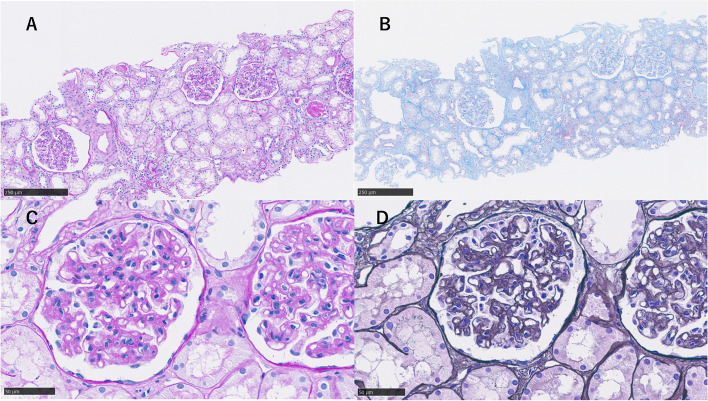
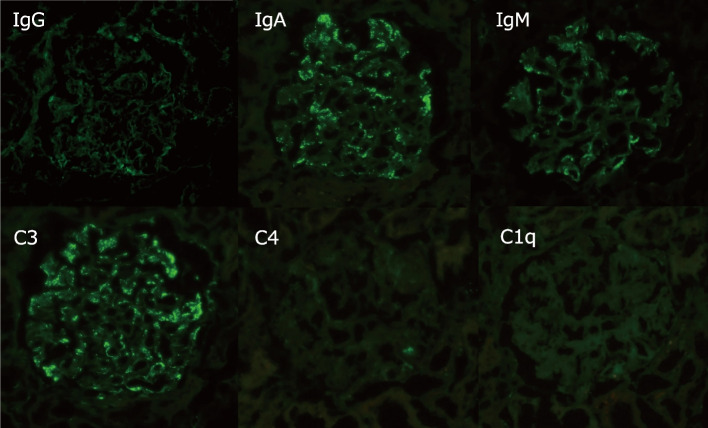
Conclusions: Although an incident of TAFRO syndrome after COVID-19 vaccination has been previously reported, this is a rare case in which the patient went into remission and was discharged. A renal biopsy was also performed in this case, which was consistent with previous reports. The favorable treatment course for TAFRO syndrome provides valuable insights.
Keywords: BNT162b2 mRNA; COVID-19; ITP (idiopathic thrombocytopenic purpura); MIS-A (multisystem inflammatory syndrome in adults); SCLS (systemic capillary leak syndrome); TAFRO syndrome.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no conflict of interest.
Figures

Similar articles
-
TAFRO syndrome with a fatal clinical course following BNT162b2 mRNA (Pfizer-BioNTech) COVID-19 vaccination: A case report.J Infect Chemother. 2022 Jul;28(7):1008-1011. doi: 10.1016/j.jiac.2022.04.005. Epub 2022 Apr 11. J Infect Chemother. 2022. PMID: 35428576 Free PMC article.
-
TAFRO syndrome with renal biopsy successfully treated with steroids and cyclosporine: a case report.BMC Nephrol. 2022 Jul 23;23(1):262. doi: 10.1186/s12882-022-02886-5. BMC Nephrol. 2022. PMID: 35870879 Free PMC article.
-
Severe systemic inflammation mimicking TAFRO syndrome following COVID-19.Int J Hematol. 2023 Sep;118(3):374-380. doi: 10.1007/s12185-023-03589-9. Epub 2023 Mar 31. Int J Hematol. 2023. PMID: 37000328 Free PMC article.
-
Successful treatment with tacrolimus in TAFRO syndrome: two case reports and literature review.Medicine (Baltimore). 2018 Jun;97(23):e11045. doi: 10.1097/MD.0000000000011045. Medicine (Baltimore). 2018. PMID: 29879072 Free PMC article. Review.
-
Recovery from prolonged thrombocytopenia in patients with TAFRO syndrome: case series and literature review.Mod Rheumatol Case Rep. 2020 Jul;4(2):302-309. doi: 10.1080/24725625.2020.1717747. Epub 2020 Feb 3. Mod Rheumatol Case Rep. 2020. PMID: 33087016 Review.
Cited by
-
TAFRO syndrome with abdominal pain as the first symptom accompanied by liver damage with hyperbilirubinemia: A case report.Heliyon. 2024 Aug 10;10(16):e36128. doi: 10.1016/j.heliyon.2024.e36128. eCollection 2024 Aug 30. Heliyon. 2024. PMID: 39229542 Free PMC article.
References
-
- Takai K, Nikkuni K, Shibuya H, Hashidate H. Thrombocytopenia with mild bone marrow fibrosis accompanied by fever, pleural effusion, ascites and hepatosplenomegaly. Rinsho Ketsueki. 2010;51:320–325. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
