

Monogenic hypertriglyceridemia and recurrent pancreatitis in a homozygous carrier of a rare APOA5 mutation: a case report
- PMID: 38872171
- PMCID: PMC11177521
- DOI: 10.1186/s13256-024-04532-0
Monogenic hypertriglyceridemia and recurrent pancreatitis in a homozygous carrier of a rare APOA5 mutation: a case report
Abstract
Background: Homozygous mutations in the APOA5 gene constitute a rare cause of monogenic hypertriglyceridemia, or familial chylomicronemia syndrome (FCS). We searched PubMed and identified 16 cases of homozygous mutations in the APOA5 gene. Severe hypertriglyceridemia related to monogenic mutations in triglyceride-regulating genes can cause recurrent acute pancreatitis. Standard therapeutic approaches for managing this condition typically include dietary interventions, fibrates, and omega-3-fatty acids. A novel therapeutic approach, antisense oligonucleotide volanesorsen is approved for use in patients with FCS.
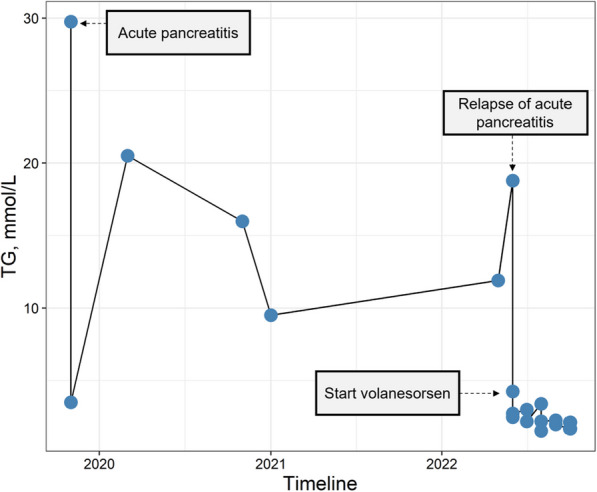
Case presentation: We report a case of a 25-years old Afghani male presenting with acute pancreatitis due to severe hypertriglyceridemia up to 29.8 mmol/L caused by homozygosity in APOA5 (c.427delC, p.Arg143Alafs*57). A low-fat diet enriched with medium-chain TG (MCT) oil and fibrate therapy did not prevent recurrent relapses, and volanesorsen was initiated. Volanesorsen resulted in almost normalized triglyceride levels. No further relapses of acute pancreatitis occurred. Patient reported an improve life quality due to alleviated chronic abdominal pain and headaches.
Conclusions: Our case reports a rare yet potentially life-threatening condition-monogenic hypertriglyceridemia-induced acute pancreatitis. The implementation of the antisense drug volanesorsen resulted in improved triglyceride levels, alleviated symptoms, and enhanced the quality of life.
Keywords: APOA5; Acute pancreatitis; Case report; Monogenic hypertriglyceridemia; Volanesorsen.
© 2024. The Author(s).
Conflict of interest statement
UM reports no conflict of interest regarding this article. WM reports grants and personal fees from Abbott Diagnostics, AMGEN, AMRYT, Boehringer Ingelheim, Sanofi, grants from Immundiagnostik GmbH, Novartis Pharma GmbH, personal fees from Vifor Pharma, and is employed with SYNLAB Holding Deutschland GmbH, outside the submitted work. OW received personal fees from AMGEN, Novartis, Sanofi, Berlin-Chemie, Sandoz, Amarin, Daiichi-Sankyo, Pfizer, Akcea Therapeutics and Sobi.
Figures
Similar articles
-
Evaluation of efficacy and safety of antisense inhibition of apolipoprotein C-III with volanesorsen in patients with severe hypertriglyceridemia.Expert Opin Pharmacother. 2020 Oct;21(14):1675-1684. doi: 10.1080/14656566.2020.1787380. Epub 2020 Jul 10. Expert Opin Pharmacother. 2020. PMID: 32646313 Review.
-
Pharmacological treatment options for severe hypertriglyceridemia and familial chylomicronemia syndrome.Expert Rev Clin Pharmacol. 2018 Jun;11(6):589-598. doi: 10.1080/17512433.2018.1480368. Epub 2018 Jun 11. Expert Rev Clin Pharmacol. 2018. PMID: 29842811 Review.
-
Familial chylomicronemia syndrome caused by 2 genetic variants in the APOA5 gene: Severe hypertriglyceridemia that complicates pregnancy.J Clin Lipidol. 2025 May-Jun;19(3):701-706. doi: 10.1016/j.jacl.2024.12.020. Epub 2025 Jan 6. J Clin Lipidol. 2025. PMID: 40023744
-
Rare Variants in Triglycerides-Related Genes Increase Pancreatitis Risk in Multifactorial Chylomicronemia Syndrome.J Clin Endocrinol Metab. 2021 Aug 18;106(9):e3473-e3482. doi: 10.1210/clinem/dgab360. J Clin Endocrinol Metab. 2021. PMID: 34019660
-
Volanesorsen for treatment of patients with familial chylomicronemia syndrome.Drugs Today (Barc). 2018 Dec;54(12):721-735. doi: 10.1358/dot.2018.54.12.2899384. Drugs Today (Barc). 2018. PMID: 30596391 Review.
Cited by
-
Unmasking a Rare Genetic Mutation: The Importance of Genetic Testing in Refractory Hypertriglyceridemia.AACE Clin Case Rep. 2024 Aug 22;10(6):240-243. doi: 10.1016/j.aace.2024.08.006. eCollection 2024 Nov-Dec. AACE Clin Case Rep. 2024. PMID: 39734502 Free PMC article.
-
Precision nutrition management in hyperlipidemia-associated acute pancreatitis: mechanistic insights and personalized therapeutic approaches.Front Nutr. 2025 Jun 18;12:1583889. doi: 10.3389/fnut.2025.1583889. eCollection 2025. Front Nutr. 2025. PMID: 40607029 Free PMC article. Review.
References
-
- Developed with the special contribution of: European Association for Cardiovascular Prevention & Rehabilitation, Authors/Task Force Members, Reiner Z, et al. ESC/EAS Guidelines for the management of dyslipidaemias: The Task Force for the management of dyslipidaemias of the European Society of Cardiology (ESC) and the European Atherosclerosis Society (EAS). Eur Heart J. 2011;32(14):1769–1818. 10.1093/eurheartj/ehr158. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
