

Exploring bi-directional impacts of Lisdexamfetamine dimesylate on psychological comorbidities and quality of life in people with Binge Eating Disorder
- PMID: 38872181
- PMCID: PMC11170888
- DOI: 10.1186/s40337-024-01041-9
Exploring bi-directional impacts of Lisdexamfetamine dimesylate on psychological comorbidities and quality of life in people with Binge Eating Disorder
Abstract
Background: Lisdexamfetamine dimesylate (LDX) has demonstrated safety and efficacy for treatment of Binge Eating Disorder (BED). However, to date, trials have not included participants with co-occurring psychiatric disorders. This study explores how LDX affects eating disorder psychopathology, symptoms of common psychiatric comorbidities of BED (ADHD, depression, anxiety), and psychological quality of life, in people with moderate to severe BED.
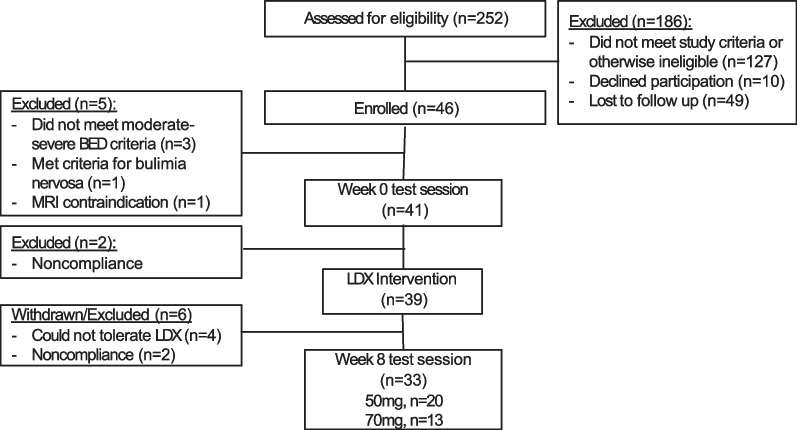
Methods: These are secondary analyses of an open-label LDX trial conducted in 41 adults (18-40 years) over eight-weeks. Participants received LDX titrated to 50 or 70 mg. Clinical assessments and self-report questionnaires were conducted at baseline and 8-week follow-up.
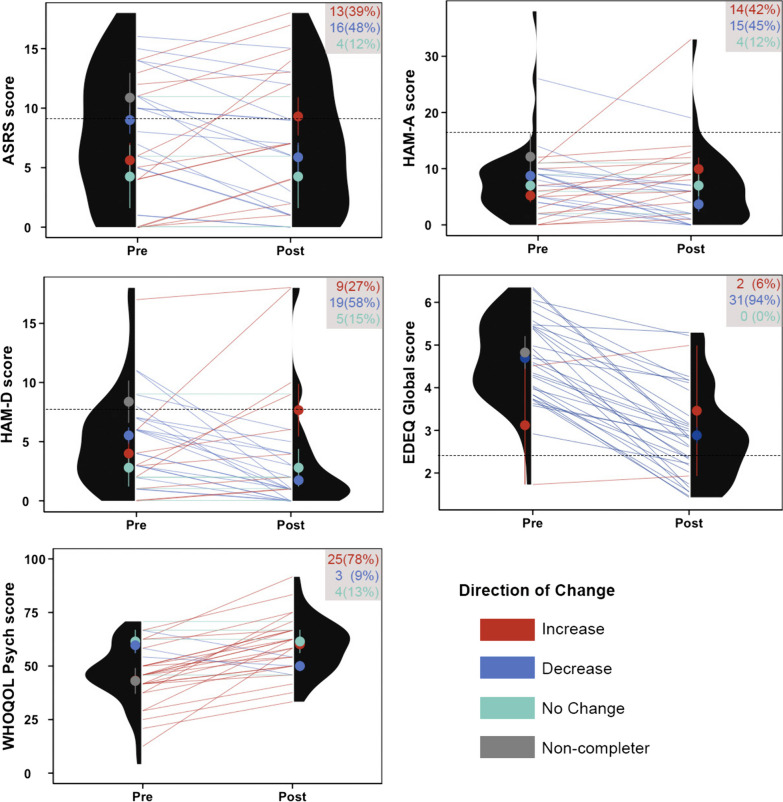
Results: Eating disorder psychopathology and psychological quality of life improved after 8-weeks of LDX. No significant group-level changes in depression, anxiety or ADHD severity scores were observed. However, the majority within the small subsets with elevated depression and ADHD symptoms experienced reduced depressive and inattentive symptom severity, respectively.
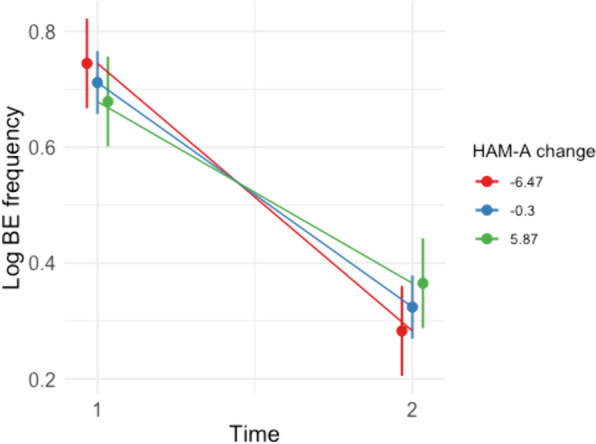
Conclusions: We provide proof-of-concept evidence that LDX may provide broader psychological benefits to individuals with BED, beyond reducing their BE frequency. Effects of LDX on anxiety should be monitored closely by clinicians. Early indications suggest that LDX may be effectively used in people with BED, with and without co-occurring psychiatric conditions, however tolerability may be lower in highly complex cases.
Trial registration: Australian and New Zealand Clinical Trials Registry (anzctr.org.au) #ACTRN12618000623291.
Keywords: ADHD; Anxiety; Depression; Medication; Mental Health; Pharmacotherapy; Psychopharmacology.
Plain language summary
Lisdexamfetamine dimesylate (LDX) has been shown to reduce binge eating frequency among those with Binge Eating Disorder (BED). However, little is known about how LDX affects symptoms of common co-occurring conditions (ADHD, depression, anxiety) and mental health more broadly. In this study, 41 people with BED received an 8-week course of LDX and their symptoms were monitored before and after treatment. Overall, people experienced a robust improvement in eating disorder psychopathology and psychological quality of life. For those with higher levels of depression and ADHD, LDX had the additional benefit of improving depressive symptoms and inattentive symptom severity, respectively. The effect of LDX on anxiety symptoms appears to be more complex, with an equal proportion of people experiencing a decrease or an increase in anxiety over the course of treatment. Those who experienced reductions in anxiety during treatment tended to have greater concurrent reductions in binge eating frequency. This study provides preliminary evidence that for people with BED, LDX may be effective at improving co-occurring symptoms of eating disorder psychopathology and psychological well-being, and potentially ADHD and depression symptoms when present at an elevated level. More research is needed among a larger sample to verify these findings.
© 2024. The Author(s).
Conflict of interest statement
PH receives/has received sessional fees and lecture fees from the Australian Medical Council, Therapeutic Guidelines publication, and HETI (New South Wales and the former NSW Institute of Psychiatry) and royalties/honoraria from Hogrefe and Huber, McGraw Hill Education, and Blackwell Scientific Publications, Biomed Central and PlosMedicine. She is Chair of the National Eating Disorders Collaboration Steering Committee in Australia (2019-) and was Member of the ICD-11 Working Group for Eating Disorders and was Chair Clinical Practice Guidelines Project Working Group (Eating Disorders) of RANZCP (2012–2015). She is a consultant to Takeda Pharmaceuticals. All views in this paper are her own. ST has been the recipient of honoraria from Shire (Takeda group of companies) for public speaking engagements and commissioned reports. He has been the Chair of their Clinical Advisory Group for Binge Eating Disorder. MRK has been the recipient of honoraria from Shire (Takeda group of companies) for public speaking engagements. SM was a one time recipient of Honoraria from Shire (Takeda) for a single public speaking engagement on an unrelated subject matter. All other authors have no potential conflicts of interest to declare.
Figures
Similar articles
-
Understanding the neural mechanisms of lisdexamfetamine dimesylate (LDX) pharmacotherapy in Binge Eating Disorder (BED): a study protocol.J Eat Disord. 2019 Jul 11;7:23. doi: 10.1186/s40337-019-0253-3. eCollection 2019. J Eat Disord. 2019. PMID: 31333843 Free PMC article.
-
Secondary outcomes and qualitative findings of an open-label feasibility trial of lisdexamfetamine dimesylate for adults with bulimia nervosa.J Eat Disord. 2023 May 22;11(1):81. doi: 10.1186/s40337-023-00796-x. J Eat Disord. 2023. PMID: 37218020 Free PMC article.
-
Impulsivity and Its Relationship With Lisdexamfetamine Dimesylate Treatment in Binge Eating Disorder.Front Psychol. 2021 Aug 31;12:716010. doi: 10.3389/fpsyg.2021.716010. eCollection 2021. Front Psychol. 2021. PMID: 34531798 Free PMC article.
-
The efficacy and safety profile of lisdexamfetamine dimesylate, a prodrug of d-amphetamine, for the treatment of attention-deficit/hyperactivity disorder in children and adults.Clin Ther. 2009 Jan;31(1):142-76. doi: 10.1016/j.clinthera.2009.01.015. Clin Ther. 2009. PMID: 19243715 Review.
-
Lisdexamfetamine: chemistry, pharmacodynamics, pharmacokinetics, and clinical efficacy, safety, and tolerability in the treatment of binge eating disorder.Expert Opin Drug Metab Toxicol. 2018 Feb;14(2):229-238. doi: 10.1080/17425255.2018.1420163. Epub 2018 Jan 4. Expert Opin Drug Metab Toxicol. 2018. PMID: 29258368 Review.
Cited by
-
Novel potential pharmacological approaches in treating eating disorders comorbid with substance use disorders.Biomed Pharmacother. 2025 Aug;189:118327. doi: 10.1016/j.biopha.2025.118327. Epub 2025 Jul 4. Biomed Pharmacother. 2025. PMID: 40616879 Review.
-
Autism, ADHD, and Their Traits in Adults With Bulimia Nervosa and Binge Eating Disorder: A Scoping Review.Eur Eat Disord Rev. 2025 Jul;33(4):647-665. doi: 10.1002/erv.3177. Epub 2025 Jan 26. Eur Eat Disord Rev. 2025. PMID: 39865514 Free PMC article.
References
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
