

Developing an optimal stratification model for colorectal cancer screening and reducing racial disparities in multi-center population-based studies
- PMID: 38872215
- PMCID: PMC11170922
- DOI: 10.1186/s13073-024-01355-y
Developing an optimal stratification model for colorectal cancer screening and reducing racial disparities in multi-center population-based studies
Abstract
Background: Early detection of colorectal neoplasms can reduce the colorectal cancer (CRC) burden by timely intervention for high-risk individuals. However, effective risk prediction models are lacking for personalized CRC early screening in East Asian (EAS) population. We aimed to develop, validate, and optimize a comprehensive risk prediction model across all stages of the dynamic adenoma-carcinoma sequence in EAS population.
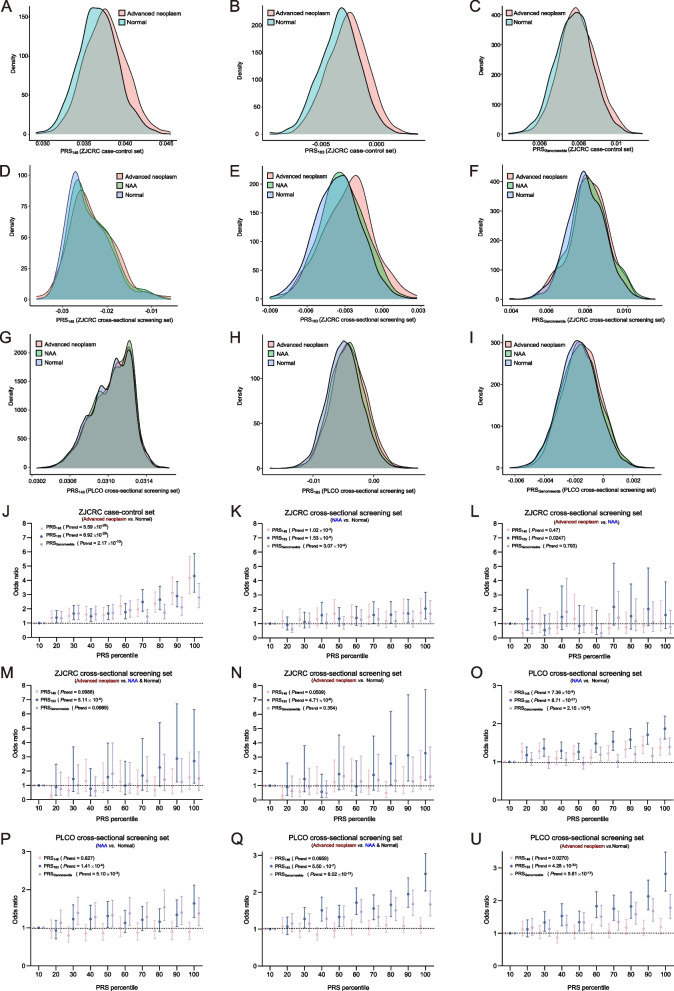
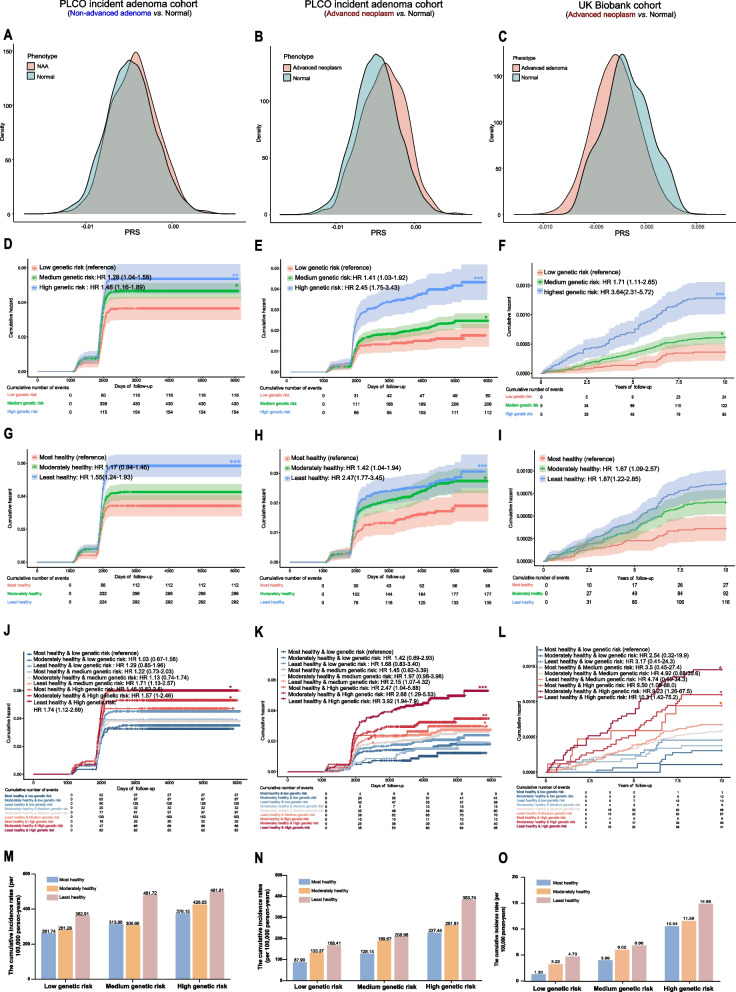
Methods: To develop precision risk-stratification and intervention strategies, we developed three trans-ancestry PRSs targeting colorectal neoplasms: (1) using 148 previously identified CRC risk loci (PRS148); (2) SNPs selection from large-scale meta-analysis data by clumping and thresholding (PRS183); (3) PRS-CSx, a Bayesian approach for genome-wide risk prediction (PRSGenomewide). Then, the performance of each PRS was assessed and validated in two independent cross-sectional screening sets, including 4600 patients with advanced colorectal neoplasm, 4495 patients with non-advanced adenoma, and 21,199 normal individuals from the ZJCRC (Zhejiang colorectal cancer set; EAS) and PLCO (the Prostate, Lung, Colorectal, and Ovarian Cancer Screening Trial; European, EUR) studies. The optimal PRS was further incorporated with lifestyle factors to stratify individual risk and ultimately tested in the PLCO and UK Biobank prospective cohorts, totaling 350,013 participants.
Results: Three trans-ancestry PRSs achieved moderately improved predictive performance in EAS compared to EUR populations. Remarkably, the PRSs effectively facilitated a thorough risk assessment across all stages of the dynamic adenoma-carcinoma sequence. Among these models, PRS183 demonstrated the optimal discriminatory ability in both EAS and EUR validation datasets, particularly for individuals at risk of colorectal neoplasms. Using two large-scale and independent prospective cohorts, we further confirmed a significant dose-response effect of PRS183 on incident colorectal neoplasms. Incorporating PRS183 with lifestyle factors into a comprehensive strategy improves risk stratification and discriminatory accuracy compared to using PRS or lifestyle factors separately. This comprehensive risk-stratified model shows potential in addressing missed diagnoses in screening tests (best NPV = 0.93), while moderately reducing unnecessary screening (best PPV = 0.32).
Conclusions: Our comprehensive risk-stratified model in population-based CRC screening trials represents a promising advancement in personalized risk assessment, facilitating tailored CRC screening in the EAS population. This approach enhances the transferability of PRSs across ancestries and thereby helps address health disparity.
Keywords: CRC early screening; Colorectal neoplasm; Lifestyle factors; Polygenic risk score; Trans-ancestry.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures



Similar articles
-
Risk assessment for colorectal cancer via polygenic risk score and lifestyle exposure: a large-scale association study of East Asian and European populations.Genome Med. 2023 Jan 24;15(1):4. doi: 10.1186/s13073-023-01156-9. Genome Med. 2023. PMID: 36694225 Free PMC article.
-
Developing and validating polygenic risk scores for colorectal cancer risk prediction in East Asians.Int J Cancer. 2022 Nov 15;151(10):1726-1736. doi: 10.1002/ijc.34194. Epub 2022 Jul 21. Int J Cancer. 2022. PMID: 35765848 Free PMC article.
-
Polygenic risk scores for the prediction of common cancers in East Asians: A population-based prospective cohort study.Elife. 2023 Mar 27;12:e82608. doi: 10.7554/eLife.82608. Elife. 2023. PMID: 36971353 Free PMC article.
-
Utility of polygenic risk scores in UK cancer screening: a modelling analysis.Lancet Oncol. 2023 Jun;24(6):658-668. doi: 10.1016/S1470-2045(23)00156-0. Epub 2023 May 10. Lancet Oncol. 2023. PMID: 37178708 Review.
-
Colorectal Cancer Risk Loci: Prognostic Factors for Clinical Outcomes? A Systematic Review and Meta-Analysis.Cancer Rep (Hoboken). 2025 May;8(5):e70230. doi: 10.1002/cnr2.70230. Cancer Rep (Hoboken). 2025. PMID: 40387276 Review.
Cited by
-
Utilization of molecular genetic approaches for colorectal cancer screening.World J Gastroenterol. 2024 Dec 14;30(46):4950-4957. doi: 10.3748/wjg.v30.i46.4950. World J Gastroenterol. 2024. PMID: 39679308 Free PMC article.
-
Plant Terpenoids in Combination with Conventional Therapeutics in Colorectal Cancer: A Promising Option.Curr Oncol Rep. 2025 Apr 21. doi: 10.1007/s11912-025-01674-2. Online ahead of print. Curr Oncol Rep. 2025. PMID: 40257647 Review.
-
Cross-cohort analysis identifies shared gut microbial signatures and validates microbial risk scores for colorectal cancer.J Transl Med. 2025 Jun 17;23(1):676. doi: 10.1186/s12967-025-06676-z. J Transl Med. 2025. PMID: 40528214 Free PMC article.
-
Lessons from national biobank projects utilizing whole-genome sequencing for population-scale genomics.Genomics Inform. 2025 Mar 6;23(1):8. doi: 10.1186/s44342-025-00040-9. Genomics Inform. 2025. PMID: 40050991 Free PMC article. Review.
-
The Genetic Variants Influencing Hypertension Prevalence Based on the Risk of Insulin Resistance as Assessed Using the Metabolic Score for Insulin Resistance (METS-IR).Int J Mol Sci. 2024 Nov 26;25(23):12690. doi: 10.3390/ijms252312690. Int J Mol Sci. 2024. PMID: 39684400 Free PMC article.
References
-
- Cardoso R, Guo F, Heisser T, Hackl M, Ihle P, De Schutter H, et al. Colorectal cancer incidence, mortality, and stage distribution in European countries in the colorectal cancer screening era: an international population-based study. Lancet Oncol. 2021;22(7):1002–1013. doi: 10.1016/S1470-2045(21)00199-6. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
- NSFC- 81925032/Distinguished Young Scholars of China
- NSFC-82130098/Key Program of National Natural Science Foundation of China
- NSFC-82073629/National Natural Science Foundation of China
- 2021YFC2500405/National Key Research and Development Program of China
- NSFC-82322058/National Science Fund for Excellent Young Scholars
- NSFC-82103929/the Program of National Natural Science Foundation of China
- NSFC-82273713/the Program of National Natural Science Foundation of China
- 2022QNRC001/Young Elite Scientists Sponsorship Program by CAST
- 2023020201010060/the Leading Talent Program of the Health Commission of Hubei Province, Knowledge Innovation Program of Wuhan
- 2042022rc0026/the Fundamental Research Funds for the Central Universities
- 2042023kf1005/the Fundamental Research Funds for the Central Universities
- WHU: 2042022kf1205/Fundamental Research Funds for the Central Universities
- WHU: 2042022kf1031/Fundamental Research Funds for the Central Universities
- whkxjsj011/Knowledge Innovation Program of Wuhan
- 2023020201020244/Knowledge Innovation Program of Wuhan
- ZNJC202207/Translational Medicine and Interdisciplinary Research Joint Fund of Zhongnan Hospital of Wuhan University
- NSFC-82003547/Youth Program of National Natural Science Foundation of China
- NSFC-82373663/Youth Program of National Natural Science Foundation of China
- WJ2023M045/Program of Health Commission of Hubei Province
LinkOut - more resources
Full Text Sources
Medical
