

Port-Site Metastasis After Laparoscopic Gastrectomy Extending to the Thigh: A Case Report
- PMID: 38872651
- PMCID: PMC11170930
- DOI: 10.7759/cureus.60273
Port-Site Metastasis After Laparoscopic Gastrectomy Extending to the Thigh: A Case Report
Abstract
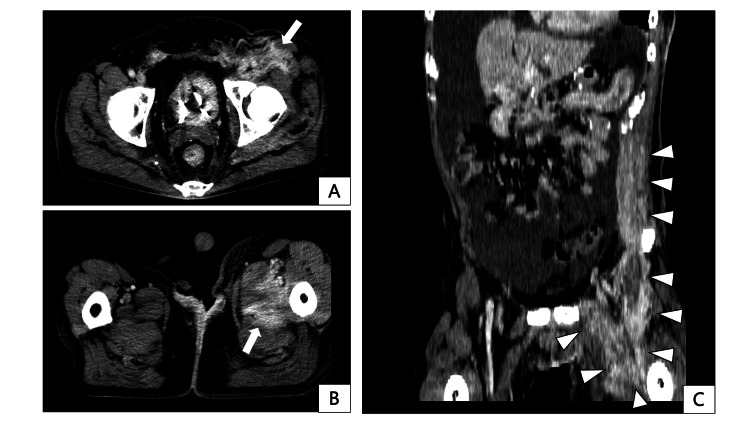
Port-site metastasis (PSM) is rare following laparoscopic gastrectomy for gastric cancer. Previous reports focused on localized lesions treated with excision; contrastingly, case reports describing extensive invasion into the lower extremity skeletal muscles causing deterioration in activities of daily living are nonexistent. A 55-year-old male underwent a laparoscopic distal gastrectomy for gastric cancer. The pathological findings revealed a stage IIIA tumor. Two years later, skin hardening was observed on the left upper abdominal wall. Computed tomography displayed a 13-cm-long, flat tumor along the skeletal muscle around the left upper 12 mm port site and right hydronephrosis. The patient was diagnosed with PSM and retroperitoneal recurrence. Despite chemotherapy, three years postoperatively, PSM widely spread from the left upper abdomen to the left thigh, eventually inducing opioid-resistant leg pain and subsequent walking difficulties. Palliative radiotherapy could not improve these symptoms. The patient died three years and five months postoperatively. Extensively invasive PSM can induce refractory cancer pain and physical disorders. Therefore, early detection and palliative resection of PSM may help maintain the quality of life of patients with gastric cancer.
Keywords: abdominal wall recurrence; gastric cancer; laparoscopic surgery; muscle metastasis; port-site recurrence.
Copyright © 2024, Goto et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures







References
-
- Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, Bray F. CA Cancer J Clin. 2021;71:209–249. - PubMed
-
- Port-site recurrence after laparoscopy-assisted gastrectomy: report of the first case. Lee YJ, Ha WS, Park ST, Choi SK, Hong SC. J Laparoendosc Adv Surg Tech A. 2007;17:455–457. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous