

A highly malignant succinate dehydrogenase A‑deficient renal cell carcinoma with bone metastasis misdiagnosed as hereditary leiomyomatosis and renal cell carcinoma: A case report
- PMID: 38872860
- PMCID: PMC11170261
- DOI: 10.3892/ol.2024.14485
A highly malignant succinate dehydrogenase A‑deficient renal cell carcinoma with bone metastasis misdiagnosed as hereditary leiomyomatosis and renal cell carcinoma: A case report
Abstract
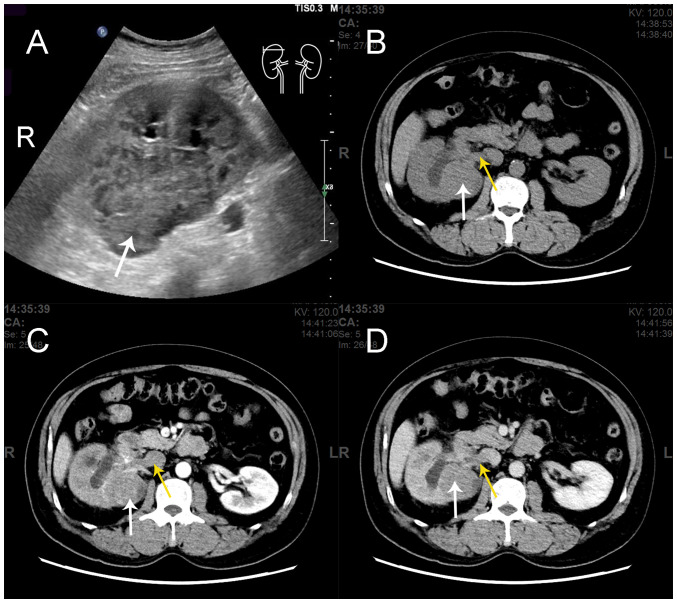
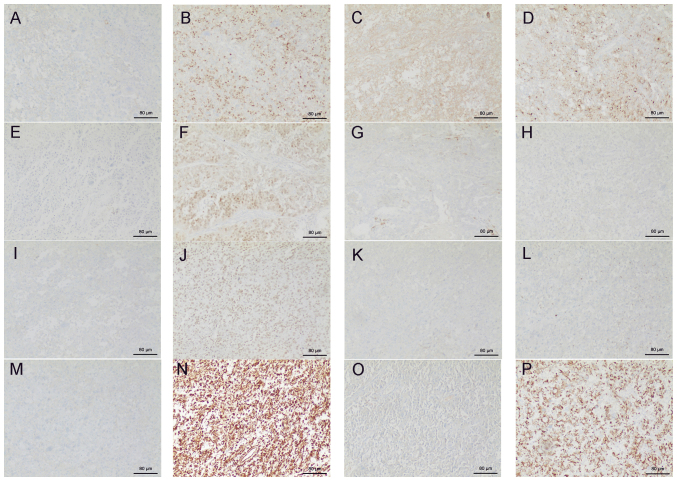
Succinate dehydrogenase (SDH)-deficient renal cell carcinoma (RCC) is an autosomal dominant syndrome caused by heterozygous pathogenic germline variants of the SDH gene. SDH mutations are associated with an increased risk of developing RCC, although studies describing SDH-deficient RCC are currently limited. The present study reported a case of SDH-deficient RCC with high malignancy and rare bone metastasis. The patient was diagnosed with a right renal mass through B-mode ultrasound imaging and showed a carcinoma embolus in the right renal vein and inferior vena cava through kidney contrast-enhanced computed tomography. A whole-body bone scan showed radionuclide accumulation in the upper end of the left humerus, which indicated possible pathological bone destruction. As a result, surgical resection was performed. The postoperative pathology indicated a high-grade RCC and although the specific classification remained uncertain, hereditary leiomyomatosis and RCC was suspected. Subsequently, a germline mutation of the succinate dehydrogenase complex flavoprotein subunit A gene was identified through high-throughput sequencing (c.1A>G, p. Met1?) and immunohistochemistry demonstrated the loss of succinate dehydrogenase complex flavoprotein subunit B expression. Postoperatively, the patient underwent radiotherapy and targeted therapy. After 6 months of follow-up treatment, there was no indication of recurrence or metastasis on thoracoabdominal CT and whole-body bone scintigraphy. Based on the present report, germline screening should potentially be encouraged in early-onset patients as family history or pathological results may not provide sufficient information for the early, differential diagnosis of SDH-deficient RCC.
Keywords: diagnose; misdiagnosed; renal cell carcinoma; succinate dehydrogenase; succinate dehydrogenase-deficient renal cell carcinoma.
Copyright: © 2024 Dai et al.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures



Similar articles
-
A distinctive, low-grade oncocytic fumarate hydratase-deficient renal cell carcinoma, morphologically reminiscent of succinate dehydrogenase-deficient renal cell carcinoma.Histopathology. 2017 Jul;71(1):42-52. doi: 10.1111/his.13183. Epub 2017 Apr 12. Histopathology. 2017. PMID: 28165631
-
Succinate dehydrogenase A deficient renal cell carcinoma: A rare renal tumor distinct from typical Succinate dehydrogenase deficient renal cell carcinoma.Pathol Res Pract. 2024 Sep;261:155459. doi: 10.1016/j.prp.2024.155459. Epub 2024 Jul 17. Pathol Res Pract. 2024. PMID: 39083879
-
Succinate Dehydrogenase Deficient Renal Cell Carcinoma With Sarcomatoid and Rhabdoid Features-A Diagnostic Dilemma.Int J Surg Pathol. 2024 Dec;32(8):1508-1513. doi: 10.1177/10668969241229333. Epub 2024 Feb 4. Int J Surg Pathol. 2024. PMID: 38311902
-
Hereditary succinate dehydrogenase-deficient renal cell carcinoma.Semin Diagn Pathol. 2024 Jan;41(1):32-41. doi: 10.1053/j.semdp.2023.11.001. Epub 2023 Nov 8. Semin Diagn Pathol. 2024. PMID: 37981479 Review.
-
Hereditary leiomyomatosis and renal cell cancer (HLRCC): Case series and review of the literature.Urol Oncol. 2021 Nov;39(11):791.e9-791.e16. doi: 10.1016/j.urolonc.2021.07.026. Epub 2021 Aug 27. Urol Oncol. 2021. PMID: 34462205 Review.
References
-
- Gill AJ, Hes O, Papathomas T, Šedivcová M, Tan PH, Agaimy A, Andresen PA, Kedziora A, Clarkson A, Toon CW, et al. Succinate dehydrogenase (SDH)-deficient renal carcinoma: A morphologically distinct entity: A clinicopathologic series of 36 tumors from 27 patients. Am J Surg Pathol. 2014;38:1588–1602. doi: 10.1097/PAS.0000000000000292. - DOI - PMC - PubMed
-
- Vanharanta S, Buchta M, McWhinney SR, Virta SK, Peçzkowska M, Morrison CD, Lehtonen R, Januszewicz A, Järvinen H, Juhola M, et al. Early-onset renal cell carcinoma as a novel extraparaganglial component of SDHB-associated heritable paraganglioma. Am J Hum Genet. 2004;74:153–159. doi: 10.1086/381054. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials