

Increased serum IL‑41 associated with acute exacerbation of chronic obstructive pulmonary disease
- PMID: 38873046
- PMCID: PMC11170319
- DOI: 10.3892/etm.2024.12601
Increased serum IL‑41 associated with acute exacerbation of chronic obstructive pulmonary disease
Abstract
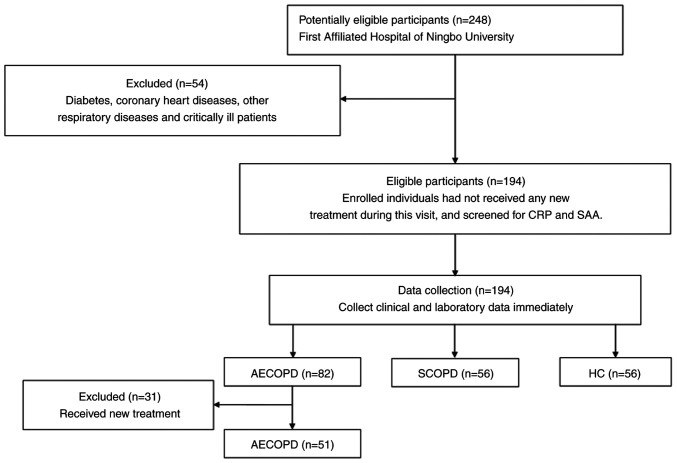
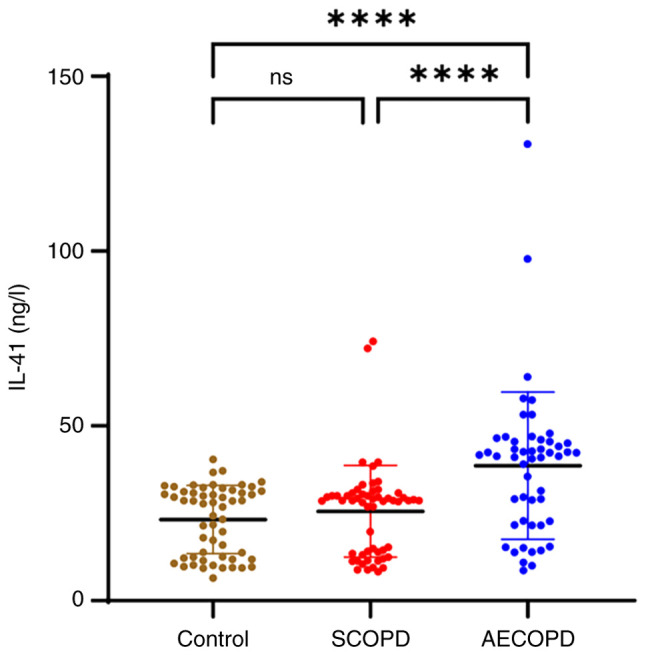
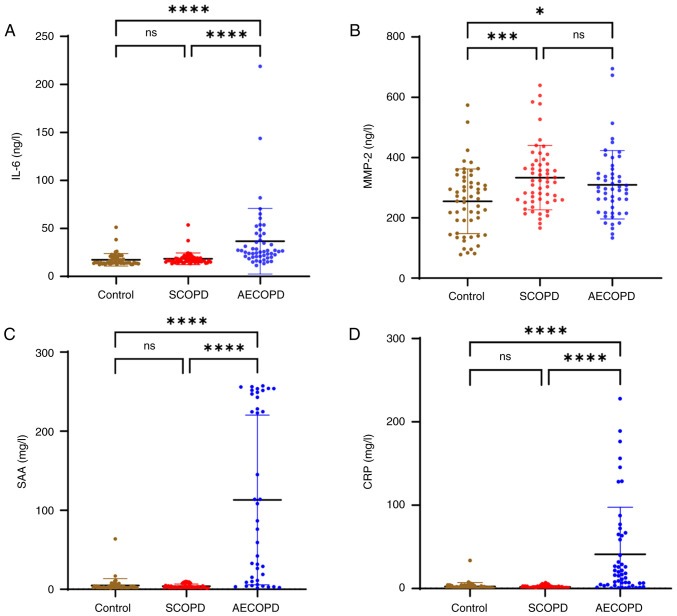
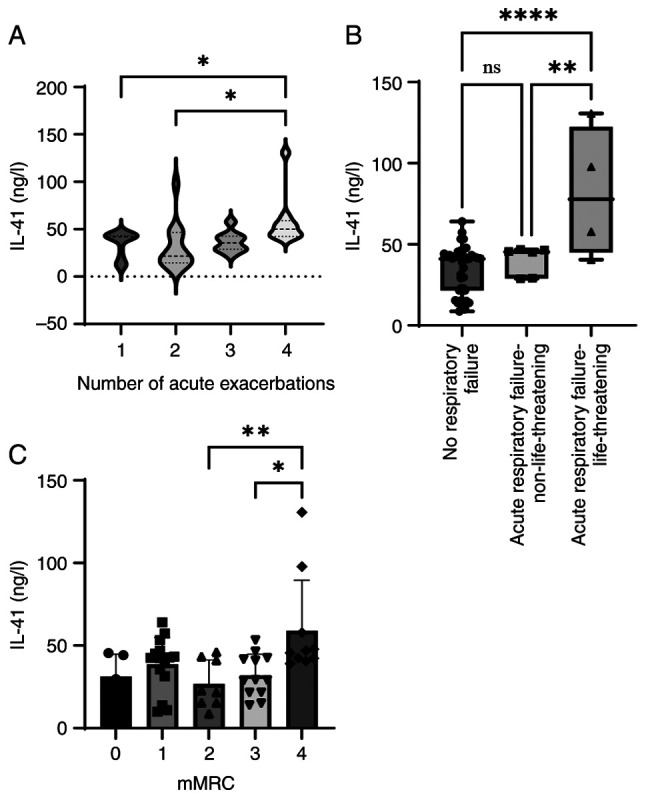
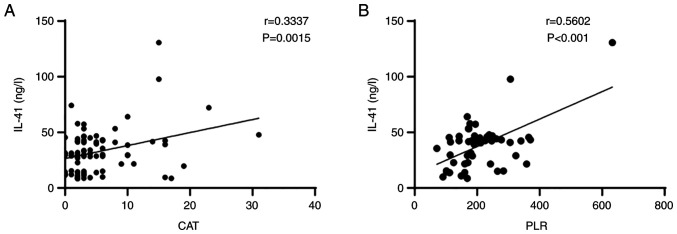
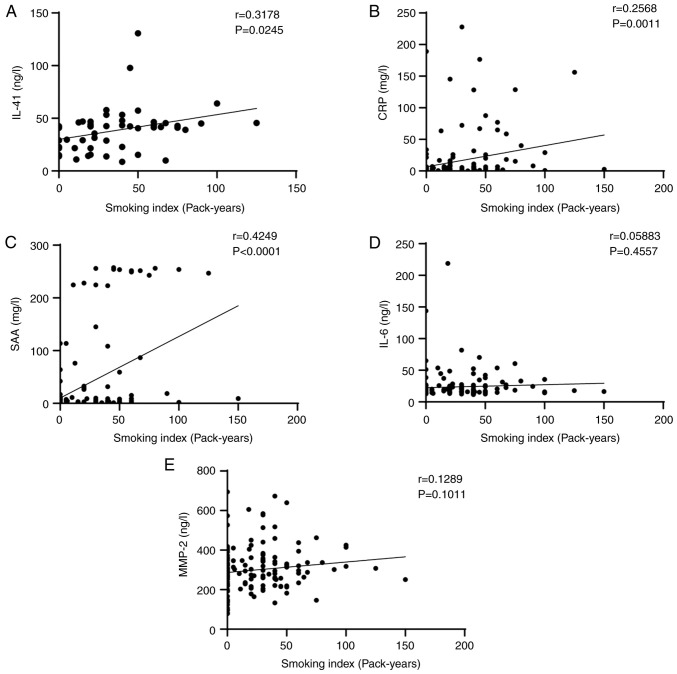
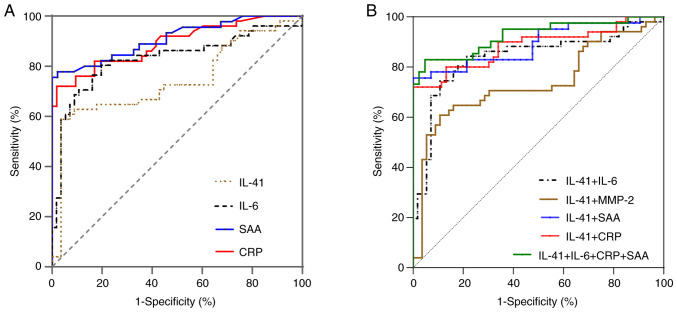
Interleukin (IL)-41 is a novel immunomodulatory cytokine involved in the pathogenesis of several inflammatory and metabolic illnesses. However, it remains unclear how IL-41 contributes to the pathogenesis of chronic obstructive pulmonary disease (COPD). Therefore, the aim of the present study was to explore the correlation between the expression level of IL-41 and acute exacerbation of COPD (AECOPD). In total, 107 patients with COPD and 56 healthy controls were recruited from the First Affiliated Hospital of Ningbo University (Ningbo, China). Serum IL-41, IL-6, and matrix metalloproteinase-2 (MMP-2) levels were evaluated using enzyme-linked immunosorbent assay. Serum amyloid A (SAA) and C-reactive protein (CRP) levels were assessed in the hospital laboratory. The levels of IL-41 were higher in the AECOPD group than in the stable COPD (SCOPD) and control groups (P<0.0001). IL-6, SAA and CRP levels, the percentage of neutrophils, as well as neutrophil-to-lymphocyte and platelet-to-lymphocyte ratios were higher in the AECOPD group than those in the SCOPD and control groups. The smoking index was positively correlated with serum IL-41, CRP and SAA levels. The expression level of IL-41 was correlated with the number of acute exacerbations, severity of the exacerbations, and COPD assessment test scores in the AECOPD group. Examination of the receiver operating characteristic (ROC) curves showed that IL-41, especially when combined with other inflammatory factors, had a specific diagnostic value for AECOPD. According to the ROC curve analysis, the area under the curve (AUC) for IL-41 was 0.742 (P=0.051), and the AUC for IL-41 combined with other inflammatory factors was 0.925 (P=0.030). Increased serum IL-41 levels were associated with AECOPD and may play a role in the monitoring and evaluation of COPD.
Keywords: C-reactive protein; acute exacerbation; chronic obstructive pulmonary disease; interleukin-41; interleukin-6; serum amyloid A.
Copyright: © 2024 Cen et al.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Dysregulated circulating microRNA-126 in chronic obstructive pulmonary disease: linkage with acute exacerbation risk, severity degree, and inflammatory cytokines.J Clin Lab Anal. 2022 Mar;36(3):e24204. doi: 10.1002/jcla.24204. Epub 2022 Jan 21. J Clin Lab Anal. 2022. PMID: 35064606 Free PMC article.
-
Circulating JNK pathway-associated phosphatase: A novel biomarker correlates with Th17 cells, acute exacerbation risk, and severity in chronic obstructive pulmonary disease patients.J Clin Lab Anal. 2022 Jan;36(1):e24153. doi: 10.1002/jcla.24153. Epub 2021 Dec 16. J Clin Lab Anal. 2022. PMID: 34918391 Free PMC article.
-
Expression and clinical significance of serum amyloid A and interleukin-6 in patients with acute exacerbation of chronic obstructive pulmonary disease.Exp Ther Med. 2020 Mar;19(3):2089-2094. doi: 10.3892/etm.2019.8366. Epub 2019 Dec 20. Exp Ther Med. 2020. PMID: 32104270 Free PMC article.
-
Correlations between serum amyloid A, C-reactive protein and clinical indices of patients with acutely exacerbated chronic obstructive pulmonary disease.J Clin Lab Anal. 2019 May;33(4):e22831. doi: 10.1002/jcla.22831. Epub 2019 Jan 21. J Clin Lab Anal. 2019. PMID: 30666727 Free PMC article.
-
Association between peripheral blood WBCs C3aR mRNA level and plasma C3a, C3aR, IL-1β concentrations and acute exacerbation of chronic obstructive pulmonary disease.Immunobiology. 2022 Jan;227(1):152164. doi: 10.1016/j.imbio.2021.152164. Epub 2021 Dec 9. Immunobiology. 2022. PMID: 34923262
Cited by
-
Interleukin 41 As A Potential Predictor of Bio-Therapy Efficacy In Patients With Rheumatoid Arthritis: A Prospective Observational Study.Int J Med Sci. 2024 Sep 30;21(13):2518-2524. doi: 10.7150/ijms.98752. eCollection 2024. Int J Med Sci. 2024. PMID: 39439456 Free PMC article.
References
-
- Celli B, Fabbri L, Criner G, Martinez FJ, Mannino D, Vogelmeier C, Montes de Oca M, Papi A, Sin DD, Han MK, Agusti A. Definition and nomenclature of chronic obstructive pulmonary disease: Time for its revision. Am J Respir Crit Care Med. 2022;206:1317–1325. doi: 10.1164/rccm.202204-0671PP. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous