

Case report: A case of bradycardia triggered by diarrhea
- PMID: 38873207
- PMCID: PMC11169780
- DOI: 10.3389/fmed.2024.1405494
Case report: A case of bradycardia triggered by diarrhea
Abstract
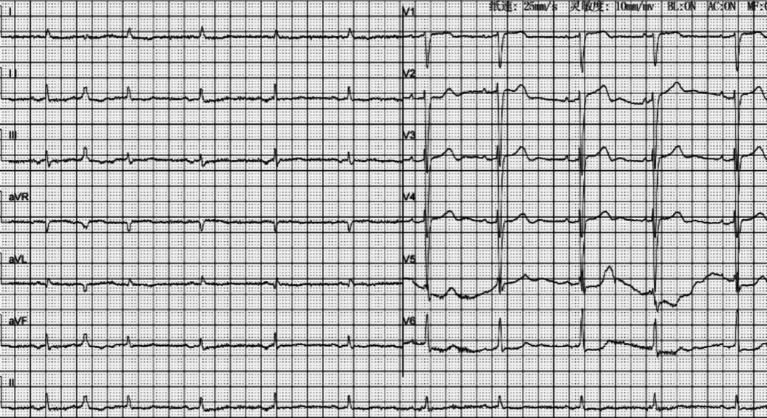
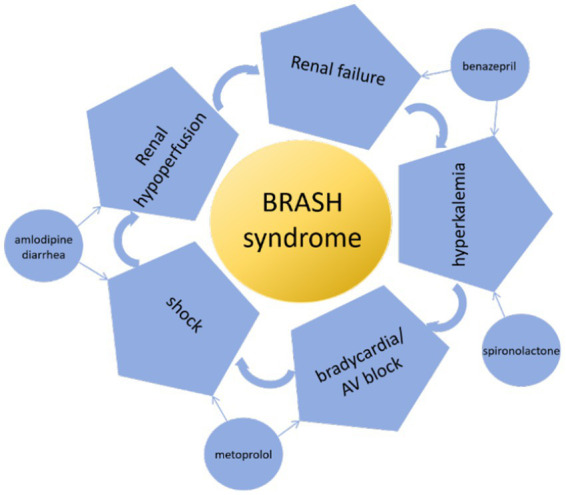
BRASH syndrome is a vicious cycle of hyperkalemia and bradycardia and is an under-recognized life-threatening clinical diagnosis. It is usually initiated by hypovolemia or hyperkalemia. We report here on the case of a 92-year-old man with hypertension and heart failure who presented to the emergency department with weakness following diarrhea. He was on amlodipine, benazepril, metoprolol, furosemide and spironolactone. The patient's blood pressure was 88/53 mmHg and the serum creatinine was 241 μmol/L. Within 2 h, the patient's heart rate decreased from 58 beats per minute to 26 beats per minute, and serum potassium levels gradually increased from 6.07 mmol/L to 7.3 mmol/L. The electrocardiogram showed a junctional escape rhythm with accidental sinus capture. The diagnosis of BRASH syndrome was made based on clinical symptoms, a biochemical profile and the results of an electrocardiogram. The patient was rapidly stabilized with the administration of intravenous calcium gluconate, dextrose and insulin, 5% sodium bicarbonate, 0.9% sodium chloride, furosemide, and oral zirconium cyclosilicate. Sinus rhythm at a heart rate of 75 bpm was detected 5 h later, along with normal serum potassium levels. After 2 weeks, kidney function returned to normal. Clinicians should be alert to patients with hyperkalemia and maintain a high index of suspicion for BRASH syndrome. Timely diagnosis and comprehensive intervention are critical for better outcomes in managing patients with BRASH.
Keywords: bradycardia; diarrhea; hyperkalemia; renal failure; shock.
Copyright © 2024 Lei, Cao, Yuan, Xiong and He.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

Similar articles
-
A BRASH Diagnosis With a Timely Intervention.Curr Probl Cardiol. 2023 Nov;48(11):101984. doi: 10.1016/j.cpcardiol.2023.101984. Epub 2023 Jul 18. Curr Probl Cardiol. 2023. PMID: 37473946
-
Bradycardia, Renal Failure, Atrioventricular (AV) Nodal Blockers, Shock, and Hyperkalemia (BRASH) Syndrome: A Confounder in the Clinical Practice.Cureus. 2024 Oct 31;16(10):e72793. doi: 10.7759/cureus.72793. eCollection 2024 Oct. Cureus. 2024. PMID: 39618623 Free PMC article.
-
BRASH syndrome with a complete heart block- a case report.BMC Cardiovasc Disord. 2024 Feb 19;24(1):114. doi: 10.1186/s12872-024-03782-6. BMC Cardiovasc Disord. 2024. PMID: 38373878 Free PMC article.
-
Clinical characteristics of BRASH syndrome: Systematic scoping review.Eur J Intern Med. 2022 Sep;103:57-61. doi: 10.1016/j.ejim.2022.06.002. Epub 2022 Jun 5. Eur J Intern Med. 2022. PMID: 35676108
-
Hyperkalemia: Pharmacotherapies and Clinical Considerations.Cureus. 2024 Jan 26;16(1):e52994. doi: 10.7759/cureus.52994. eCollection 2024 Jan. Cureus. 2024. PMID: 38406030 Free PMC article. Review.
Cited by
-
Adverse events associated with amlodipine: a pharmacovigilance study using the FDA adverse event reporting system.Front Cardiovasc Med. 2025 May 6;12:1504671. doi: 10.3389/fcvm.2025.1504671. eCollection 2025. Front Cardiovasc Med. 2025. PMID: 40395720 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources