

Start, switch and stop (triple-S) criteria for enzyme replacement therapy of late-onset Pompe disease: European Pompe Consortium recommendation update 2024
- PMID: 38873957
- PMCID: PMC11295151
- DOI: 10.1111/ene.16383
Start, switch and stop (triple-S) criteria for enzyme replacement therapy of late-onset Pompe disease: European Pompe Consortium recommendation update 2024
Abstract
Background and purpose: Two novel enzyme replacement therapies (ERTs), studied in phase 3 trials in late-onset Pompe patients, reached marketing authorization by the European Medicines Agency in 2022 and 2023. The European Pompe Consortium (EPOC) updates and extends the scope of the 2017 recommendations for starting, switching and stopping ERT.
Methods: The European Pompe Consortium consists of 25 neuromuscular and metabolic experts from eight European countries. This update was performed after an in-person meeting, three rounds of discussion and voting to provide a consensus recommendation.
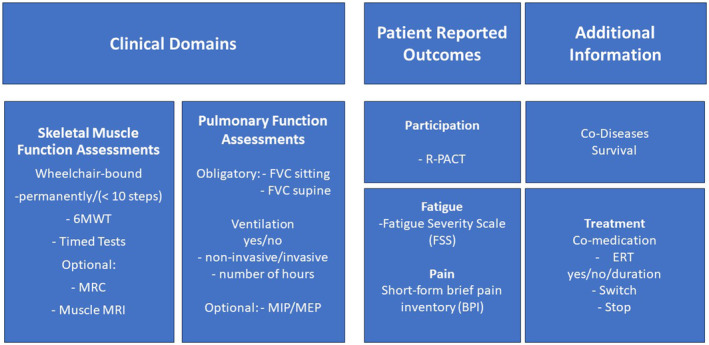
Results: The patient should be symptomatic, that is, should have skeletal muscle weakness or respiratory muscle involvement. Muscle magnetic resonance imaging findings showing substantial fat replacement can support the decision to start in a patient-by-patient scenario. Limited evidence supports switching ERT if there is no indication that skeletal muscle and/or respiratory function have stabilized or improved during standard ERT of 12 months or after severe infusion-associated reactions. Switching of ERT should be discussed on a patient-by-patient shared-decision basis. If there are severe, unmanageable infusion-associated reactions and no stabilization in skeletal muscle function during the first 2 years after starting or switching treatment, stopping ERT should be considered. After stopping ERT for inefficacy, restarting ERT can be considered. Six-monthly European Pompe Consortium muscle function assessments are recommended.
Conclusions: The triple-S criteria on ERT start, switch and stop include muscle magnetic resonance imaging as a supportive finding and the potential option of home infusion therapy. Six-monthly long-term monitoring of muscle function is highly recommended to cover insights into the patient's trajectory under ERT.
Keywords: EPOC; Pompe disease; enzyme replacement therapy; late‐onset; therapy switch.
© 2024 The Author(s). European Journal of Neurology published by John Wiley & Sons Ltd on behalf of European Academy of Neurology.
Conflict of interest statement
This article and its recommendations were developed independently of the pharmaceutical industry. Esther Brusse has no relevant conflicts of interest. Jordi Diaz‐Manera has received research grants from Spark, Sarepta, Sanofi and Boehringer Ingelheim and payments for consultancy or as speaker from Amicus Therapeutics, Astellas, Sanofi, Sarepta, Lupin and Boehringer Ingelheim and payments for consultancy or as a speaker from Amicus Therapeutics, Astellas, Sanofi, Sarepta, Lupin and Spark. He declares no stocks or shares. Andreas Hahn has received honoraria from Sanofi‐Aventis and Amicus as an advisory board member and for lectures. He declares no stocks or shares. Pascal Laforet has received research grants from Amicus Therapeutics Inc. and Sanofi, AMDA Foundation, Association Francophone des Glycogénoses, Vaincre les Maladies Lysosomales (VML) and speaker's honoraria from Amicus Therapeutics Inc. and Sanofi. He has participated as a scientific advisor for Amicus Therapeutics Inc., Sanofi and Spark Therapeutics. He declares no stocks or shares. Cornelia Kornblum has received speaker's honoraria and/or travel funding from Chiesi, Amicus Therapeutics, Fulcrum Therapeutics, Novartis, Sanofi and Santhera. She acknowledges financial support as an advisory board member and/or primary investigator for Amicus Therapeutics, Fulcrum Therapeutics, Hormosan, Reneo Pharmaceuticals, Roche Pharma AG, Sanofi and Stealth BioTherapeutics. She declares no stocks or shares. Eugen Mengel received research grants, speakers' fees and consulting honoraria from Sanofi, Orphazyme, Takeda, Cyclo Therapeutics, Idorsia, JCR, Denali, Amicus and Avrobio. Tiziana Mongini has received honoraria from Sanofi‐Aventis and Amicus as an advisory board member and for lectures. She received financial support for educational activities from Sanofi, Biogen and Roche. She declares no stocks or shares. David Orlikowski was an investigator for Amicus Therapeutics Inc. and Spark Therapeutics. He has participated as a scientific advisor for Spark Therapeutics. He declares no stocks or shares. W. W. M. Pim Pijnappel is an advisor of LentiCure B.V. Thomas Scherer has received an investigator‐initiated research grant from Sanofi and speaker's honoraria from Amicus Therapeutics and Sanofi. He has participated as a scientific advisor for Amicus Therapeutics and Sanofi. He declares no stocks or shares. Benedikt Schoser has received unrestricted research grants from Amicus, Astellas, Roche diagnostics, Marigold Foundation, AMDA Foundation and speaker's honoraria from Amicus Therapeutics Inc., Alexion, Kedrion and Sanofi. He has participated as a scientific advisor for Amicus, Argenx, Astellas, Bayer, Pepgen, Sanofi, Spark and Taysha. He declares no stocks or shares. Nadine A. M. E. van der Beek has participated in advisory board meetings for Sanofi and Bayer and has received speaker honoraria from Sanofi under agreements between Erasmus MC University Medical Center and the relevant industry. Pieter A. van Doorn has received unrestricted research grants from the Prinses Beatrix Spierfonds and Sanquin Blood Supply. He participated as a scientific advisor/steering committee member for Annexon, Argenx, Hansa, Octapharma, Roche, and Sanofi Genzyme, all for indications other than Pompe disease. All payments were made to Erasmus MC University Medical Center. He has no relevant conflicts of interest. Johanna van den Hout has participated in advisory board meetings for Sanofi and has received speaker honoraria from Sanofi and Amicus under agreements between Erasmus MC University Medical Center and the relevant industry. John Vissing has acted as a consultant for Amicus Therapeutics, Argenx BVBA, Arvinas, Atamyo Therapeutics, Biogen, Dyne Therapeutics, Fulcrum Therapeutics, Horizon Therapeutics, Lupin, ML Biopharma, Regeneron, Roche, Sanofi Genzyme, Sarepta Therapeutics and UCB Biopharma SPRL. He has received research grants, travel support, and/or speaker fees from Alexion, AstraZeneca Rare Disease, Edgewise Therapeutics, Fulcrum Therapeutics, Horizon Therapeutics, Sanofi Genzyme and UCB Biopharma SPRL. Ans T. van der Ploeg has acted as advisor and participated in clinical trials, registries and/or investigational projects for Amicus Therapeutics, Alexion, AskBio, Astellas, Bayer, Biogen, Biomarin, Chiesi, Denali, Dynacure, Pharming, Sarepta, Sanofi Genzyme, Ultragenix under agreements between the industry and Erasmus MC University Medical Center. All other authors declare no financial or other conflicts of interest.
Figures
References
-
- van der Ploeg AT, Kruijshaar ME, Toscano A, et al. European consensus for starting and stopping enzyme replacement therapy in adult patients with Pompe disease: a 10‐year experience. Eur J Neurol. 2017;24(768):e31. - PubMed
-
- Schoser B, Laforêt P, Kruijshaar ME, et al. 208th ENMC International Workshop: formation of a European Network to develop a European data sharing model and treatment guidelines for Pompe disease Naarden, The Netherlands, 26–28 September 2014. Neuromuscul Disord. 2015;25(8):674‐678. - PubMed
-
- Diaz‐Manera J, Kishnani PS, Kushlaf H, et al. Safety and efficacy of avalglucosidase alfa versus alglucosidase alfa in patients with late‐onset Pompe disease (COMET): a phase 3, randomised, multicentre trial. Lancet Neurol. 2021;20(12):1012‐1026. Erratum in: Lancet Neurol. 2022;21(4):e4. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
