

Efficacy and safety of robotic vs. laparoscopic gastrectomy for patients with gastric cancer: systematic review and meta-analysis
- PMID: 38874467
- PMCID: PMC11634110
- DOI: 10.1097/JS9.0000000000001826
Efficacy and safety of robotic vs. laparoscopic gastrectomy for patients with gastric cancer: systematic review and meta-analysis
Abstract
Background: The emergence of robotic surgical systems compensated for the technological shortcomings of laparoscopic approaches. However, whether robotic gastrectomy (RG) has better perioperative outcomes and survival than laparoscopic gastrectomy (LG) for gastric cancer (GC) is still unclear but increasingly drawing attention.
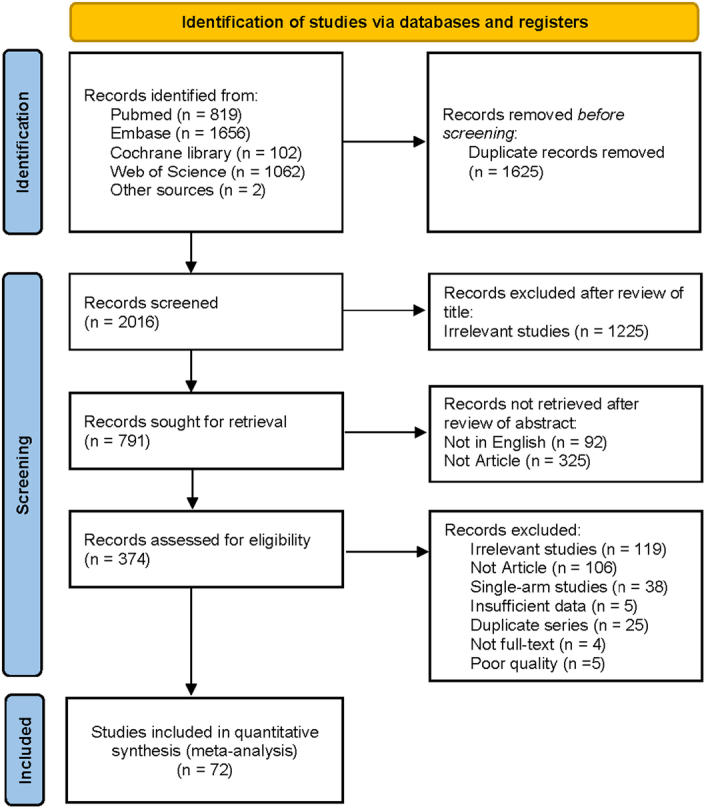
Materials and methods: In this systematic review and meta-analysis, we searched PubMed, EMBASE, Web of Science, and Cochrane Library as of 20 January 2024, and referenced a list of eligible articles for all published studies comparing RG and LG for patients with GC. Data on study characteristics, individual characteristics, and outcome parameters were extracted. The quality of studies was assessed using the Revised Cochrane risk-of-bias 2 tool and the risk of bias in nonrandomized studies of interventions tool. The main outcome measures were overall survival (OS) and disease-free survival (DFS).
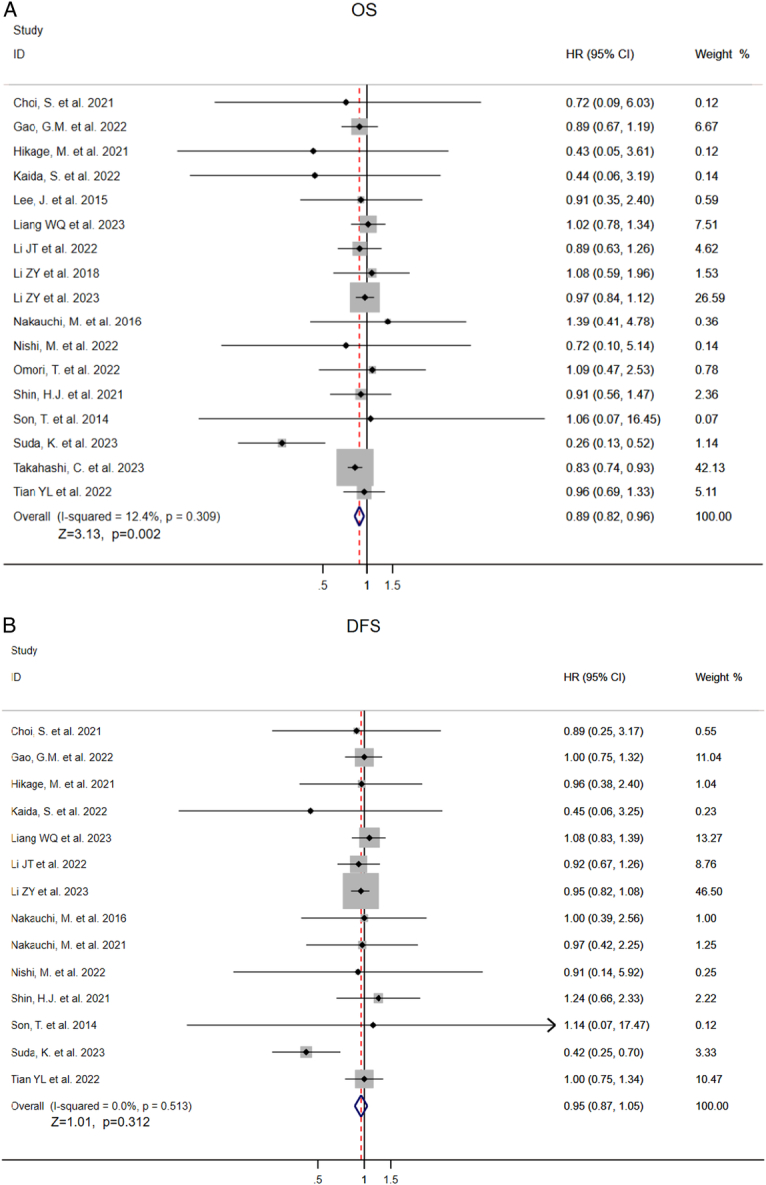
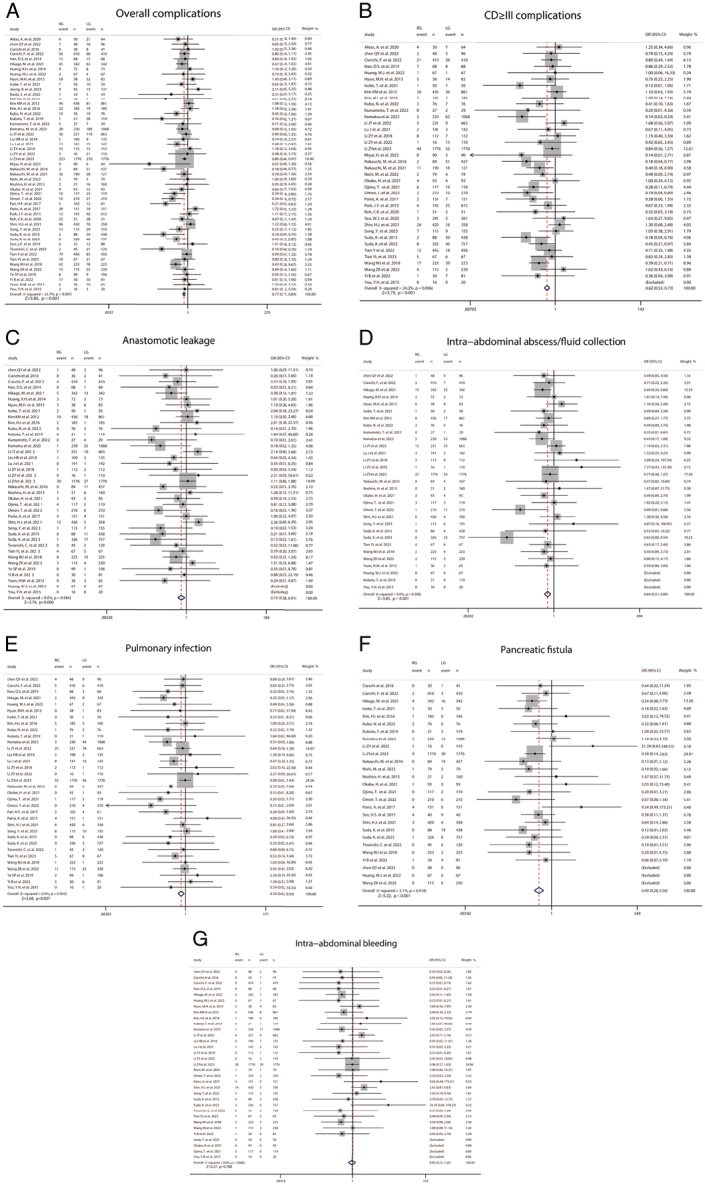
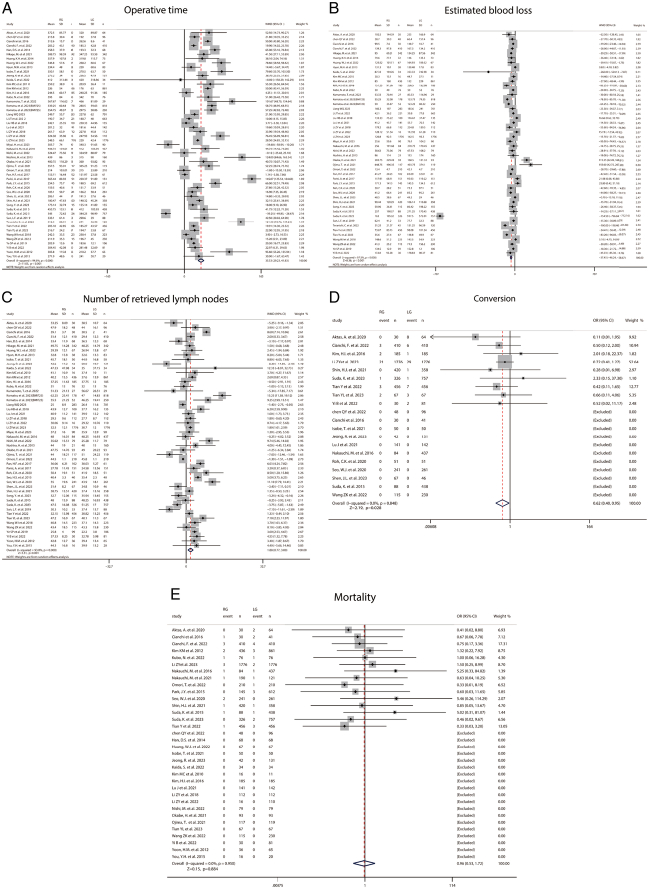
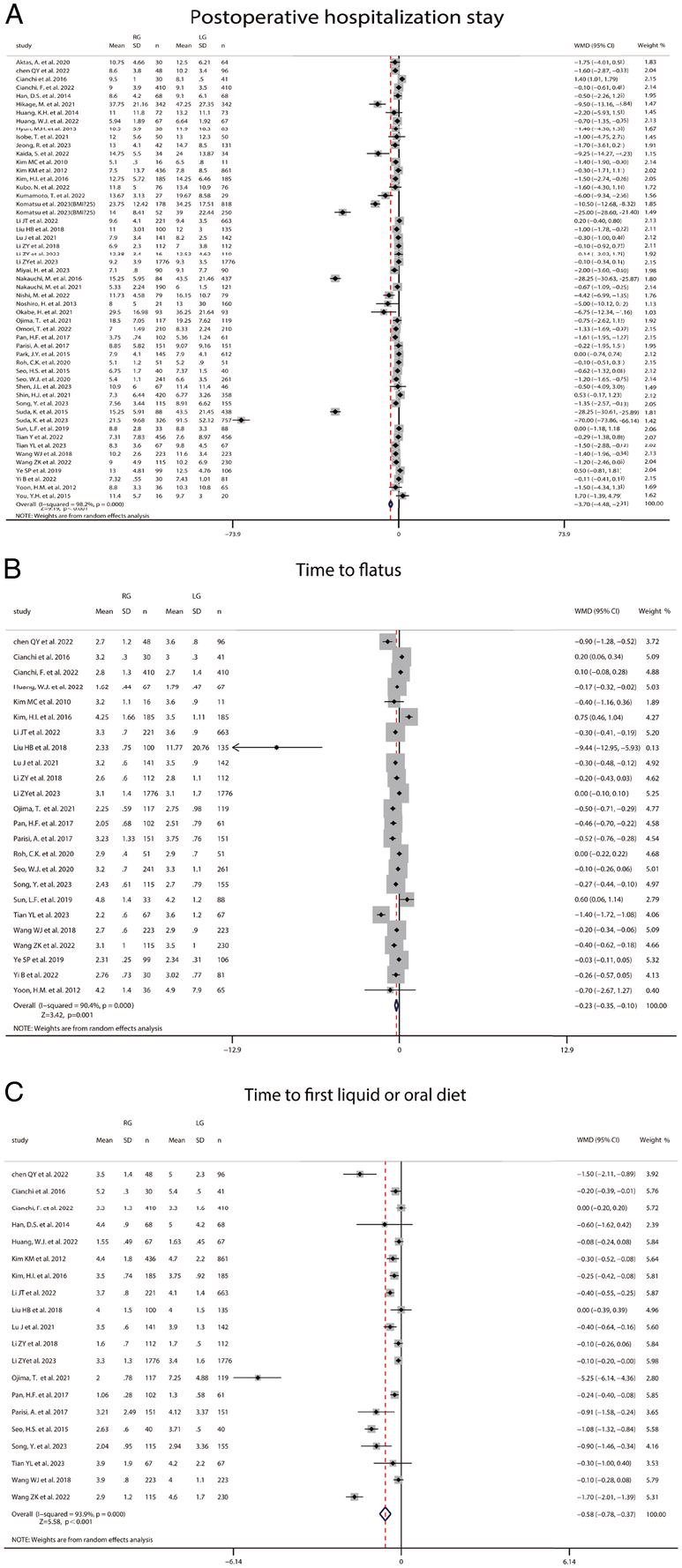
Results: The authors identified 3641 articles, of which 72 studies (30 081 patients) were included in the meta-analysis. Compared with LG, RG was associated with higher OS [hazard ratio (HR)=0.89, 95% CI=0.83-0.96], lower rate of overall postoperative complications [odds ratio (OR)=0.77, 95% CI=0.71-0.84], longer operating time [mean difference (MD)=35.53, 95% CI=29.23-41.83], less estimated blood loss (MD=-37.45, 95% CI=-46.24 to -28.67), a higher number of retrieved lymph nodes (MD=1.88, 95% CI=0.77-3.00), faster postoperative recovery, and lower rate of conversion (OR=0.44, 95% CI=0.36-0.55). Mortality and DFS were not significantly different between the two groups. The subgroup of meta-analysis results also showed the advantages of robotic surgery over laparoscopic surgery in intracorporeal reconstruction, total gastrectomy, Ⅰ/Ⅱ stage, and BMI≥25, especially for patients with stage Ⅰ/Ⅱ, there are better OS and DFS.
Conclusion: Our findings point to robotic surgery having great benefits compared with laparoscopic surgery in GC. Our study may help inform decision-making in applying robotic surgical systems to clinical treatment.
Copyright © 2024 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors declare no conflicts of interest.
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
Figures
Similar articles
-
Robotic versus laparoscopic gastrectomy for gastric cancer: The largest meta-analysis.Int J Surg. 2020 Oct;82:210-228. doi: 10.1016/j.ijsu.2020.07.053. Epub 2020 Aug 12. Int J Surg. 2020. PMID: 32800976 Review.
-
Comparative analysis of robotic gastrectomy and laparoscopic gastrectomy for gastric cancer in terms of their long-term oncological outcomes: a meta-analysis of 3410 gastric cancer patients.World J Surg Oncol. 2019 May 23;17(1):86. doi: 10.1186/s12957-019-1628-2. World J Surg Oncol. 2019. PMID: 31122260 Free PMC article.
-
Effectiveness and safety of robotic versus traditional laparoscopic gastrectomy for gastric cancer: An updated systematic review and meta-analysis.J Cancer Res Ther. 2019;15(7):1450-1463. doi: 10.4103/jcrt.JCRT_798_18. J Cancer Res Ther. 2019. PMID: 31939422
-
Comparison of short- and long-term outcomes of robotic versus laparoscopic gastrectomy for locally advanced gastric cancer after neoadjuvant therapy: a high-volume center retrospective study with propensity score matching.Surg Endosc. 2025 May;39(5):2814-2827. doi: 10.1007/s00464-025-11626-3. Epub 2025 Mar 10. Surg Endosc. 2025. PMID: 40064692
-
Robotic versus laparoscopic gastrectomy for gastric cancer: a systematic review and meta-analysis.World J Surg Oncol. 2020 Nov 24;18(1):306. doi: 10.1186/s12957-020-02080-7. World J Surg Oncol. 2020. PMID: 33234134 Free PMC article.
Cited by
-
Short-term outcomes of robotic versus laparoscopic gastrectomy for proximal gastric cancer: a systematic review and meta-analysis of propensity score-matched or baseline-balanced retrospective studies.J Robot Surg. 2025 Jun 23;19(1):318. doi: 10.1007/s11701-025-02415-0. J Robot Surg. 2025. PMID: 40549062
-
Robotic pancreatoduodenectomy provides better short-term outcomes as compared to its laparoscopic counterpart: a meta-analysis.Front Oncol. 2025 Jun 18;15:1568957. doi: 10.3389/fonc.2025.1568957. eCollection 2025. Front Oncol. 2025. PMID: 40606993 Free PMC article.
-
Evaluating the Role of Robotic Surgery Gastric Cancer Treatment: A Comprehensive Review by the Robotic Global Surgical Society (TROGSS) and European Federation International Society for Digestive Surgery (EFISDS) Joint Working Group.Curr Oncol. 2025 Jan 31;32(2):83. doi: 10.3390/curroncol32020083. Curr Oncol. 2025. PMID: 39996883 Free PMC article. Review.
-
Robotic versus laparoscopic pancreaticoduodenectomy for pancreatic and periampullary tumors: a meta-analysis.Front Oncol. 2024 Nov 19;14:1486504. doi: 10.3389/fonc.2024.1486504. eCollection 2024. Front Oncol. 2024. PMID: 39629002 Free PMC article.
References
-
- Sung H, Ferlay J, Siegel RL, et al. . Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2021;71:209–249. - PubMed
-
- Bang YJ, Kim YW, Yang HK, et al. . Adjuvant capecitabine and oxaliplatin for gastric cancer after D2 gastrectomy (CLASSIC): a phase 3 open-label, randomised controlled trial. Lancet 2012;379:315–321. - PubMed
-
- Cats A, Jansen EPM, van Grieken NCT, et al. . Chemotherapy versus chemoradiotherapy after surgery and preoperative chemotherapy for resectable gastric cancer (CRITICS): an international, open-label, randomised phase 3 trial. Lancet Oncol 2018;19:616–628. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
