

Fragment size of lateral Hoffa fractures determines screw fixation trajectory: a human cadaveric cohort study
- PMID: 38874493
- PMCID: PMC11177862
- DOI: 10.2340/17453674.2024.40841
Fragment size of lateral Hoffa fractures determines screw fixation trajectory: a human cadaveric cohort study
Abstract
Background and purpose: Recommendations regarding fragment-size-dependent screw fixation trajectory for coronal plane fractures of the posterior femoral condyles (Hoffa fractures) are lacking. The aim of this study was to compare the biomechanical properties of anteroposterior (AP) and crossed posteroanterior (PA) screw fixations across differently sized Hoffa fractures on human cadaveric femora.
Patients and methods: 4 different sizes of lateral Hoffa fractures (n = 12 x 4) were created in 48 distal human femora according to the Letenneur classification: (i) type I, (ii) type IIa, (ii) type IIb, and (iv) type IIc. Based on bone mineral density (BMD), specimens were assigned to the 4 fracture clusters and each cluster was further assigned to fixation with either AP (n = 6) or crossed PA screws (n = 6) to ensure homogeneity of BMD values and comparability between the different test conditions. All specimens were biomechanically tested under progressively increasing cyclic loading until failure, capturing the interfragmentary movements via motion tracking.
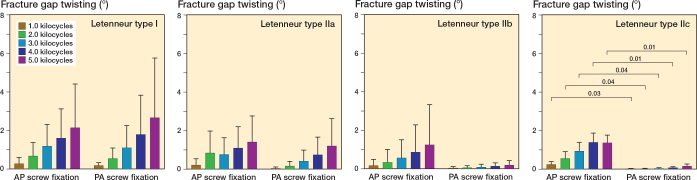
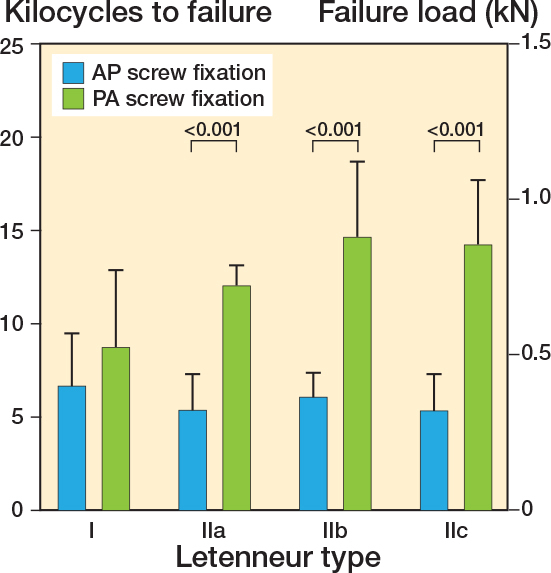
Results: For Letenneur type I fractures, kilocycles to failure (mean difference [∆] 2.1, 95% confidence interval [CI] -1.3 to 5.5), failure load (∆ 105 N, CI -83 to 293), axial displacement (∆ 0.3 mm, CI -0.8 to 1.3), and fragment rotation (∆ 0.5°, CI -3.2 to 2.1) over 5.0 kilocycles did not differ significantly between the 2 screw trajectories. For each separate subtype of Letenneur type II fractures, fixation with crossed PA screws resulted in significantly higher kilocycles to failure (∆ 6.7, CI 3.3-10.1 to ∆ 8.9, CI 5.5-12.3) and failure load (∆ 275 N, CI 87-463 to ∆ 438, CI 250-626), as well as, less axial displacement from 3.0 kilocycles onwards (∆ 0.4°, CI 0.03-0.7 to ∆ 0.5°, CI 0.01-0.9) compared with AP screw fixation.
Conclusion: Irrespective of the size of Letenneur type II fractures, crossed PA screw fixation provided greater biomechanical stability than AP-configured screws, whereas both screw fixation techniques demonstrated comparable biomechanical competence for Letenneur type I fractures. Fragment-size-dependent treatment strategies might be helpful to determine not only the screw configuration but also the surgical approach.
Figures






Similar articles
-
Plate-augmented fixation of comminuted Letenneur type II Hoffa fractures provides favorable stability compared to isolated posteroanterior screw fixation - a biomechanical study.Arch Orthop Trauma Surg. 2025 May 19;145(1):301. doi: 10.1007/s00402-025-05920-x. Arch Orthop Trauma Surg. 2025. PMID: 40387941 Free PMC article.
-
Plate fixation for Letenneur type I Hoffa fracture: a biomechanical study.Injury. 2017 Jul;48(7):1492-1498. doi: 10.1016/j.injury.2017.03.044. Epub 2017 Mar 30. Injury. 2017. PMID: 28390685
-
A biomechanical comparison of two screw fixation methods in a Letenneur type I Hoffa fracture.BMC Musculoskelet Disord. 2020 Jul 28;21(1):497. doi: 10.1186/s12891-020-03527-4. BMC Musculoskelet Disord. 2020. PMID: 32723376 Free PMC article.
-
The effect of screw orientation on internal fixation of Letenneur type II Hoffa fractures: a biomechanics study.BMC Musculoskelet Disord. 2024 Feb 2;25(1):107. doi: 10.1186/s12891-024-07222-6. BMC Musculoskelet Disord. 2024. PMID: 38308240 Free PMC article.
-
Busch-Hoffa fracture: A systematic review.Medicine (Baltimore). 2023 Dec 1;102(48):e36161. doi: 10.1097/MD.0000000000036161. Medicine (Baltimore). 2023. PMID: 38050206 Free PMC article.
Cited by
-
Novel CT-based classification of Hoffa fracture and optimal treatment strategies.Front Surg. 2025 May 26;12:1564933. doi: 10.3389/fsurg.2025.1564933. eCollection 2025. Front Surg. 2025. PMID: 40491427 Free PMC article.
-
Plate-augmented fixation of comminuted Letenneur type II Hoffa fractures provides favorable stability compared to isolated posteroanterior screw fixation - a biomechanical study.Arch Orthop Trauma Surg. 2025 May 19;145(1):301. doi: 10.1007/s00402-025-05920-x. Arch Orthop Trauma Surg. 2025. PMID: 40387941 Free PMC article.
References
-
- Onay T, Gulabi D, Colak I, Bulut G, Gumustas S A, Cecen G S. Surgically treated Hoffa Fractures with poor long-term functional results. Injury 2018; 49: 398-403. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
