

The REMAR (Rhein-Main-Registry) real-world study: prospective evaluation of the 21-gene breast recurrence score® assay in addition to Ki-67 for adjuvant treatment decisions in early-stage breast cancer
- PMID: 38874685
- PMCID: PMC11297120
- DOI: 10.1007/s10549-024-07390-y
The REMAR (Rhein-Main-Registry) real-world study: prospective evaluation of the 21-gene breast recurrence score® assay in addition to Ki-67 for adjuvant treatment decisions in early-stage breast cancer
Abstract
Purpose: Ki-67 is recommended by international/national guidelines for risk stratification in early breast cancer (EBC), particularly for defining "intermediate risk," despite inter-laboratory/inter-observer variability and cutoff uncertainty. We investigated Ki-67 (> 10%- < 40%, determined locally) as a prognostic marker for intermediate/high risk in EBC, pN0-1 patients.
Methods: This prospective, non-interventional, real-world study included females ≥ 18 years, with pN0/pN1mi/pN1, HR+ , HER2-negative EBC, and locally determined Ki-67 ranging 10%-40%. The primary outcome was changes in treatment recommendations after disclosing the Oncotype DX Breast Recurrence Score®(RS) assay result.
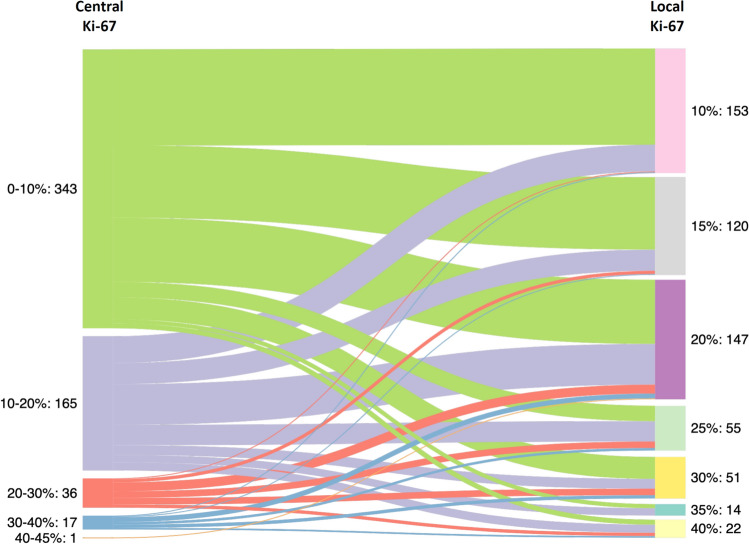
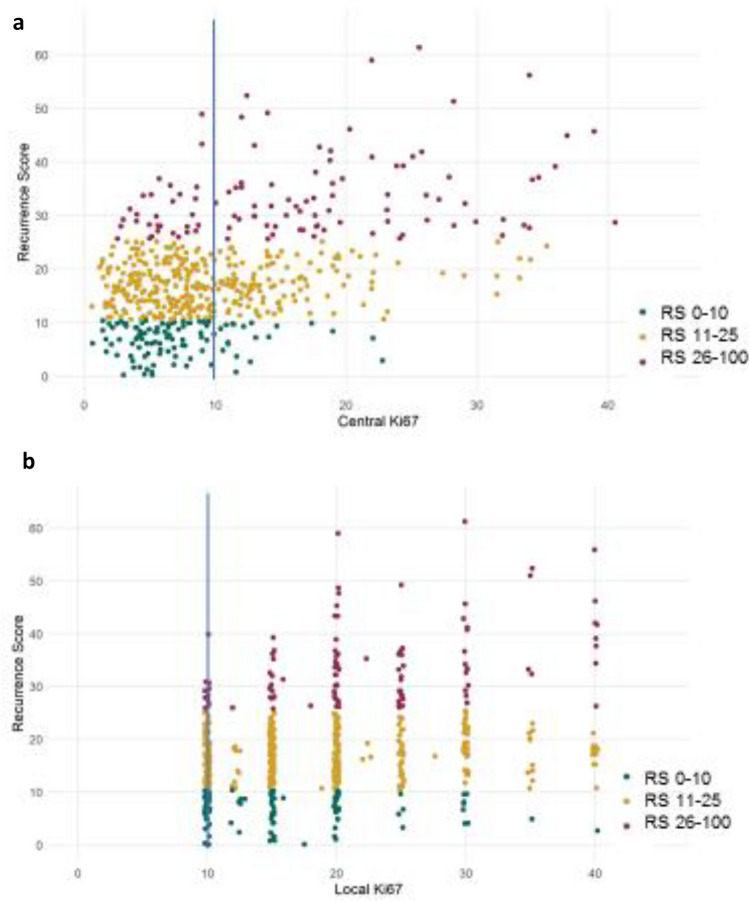
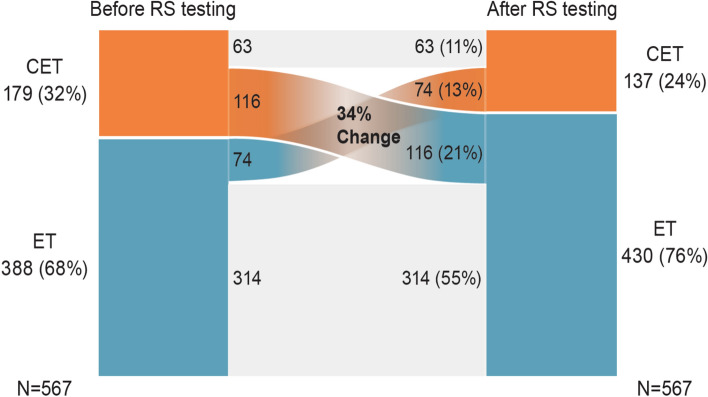
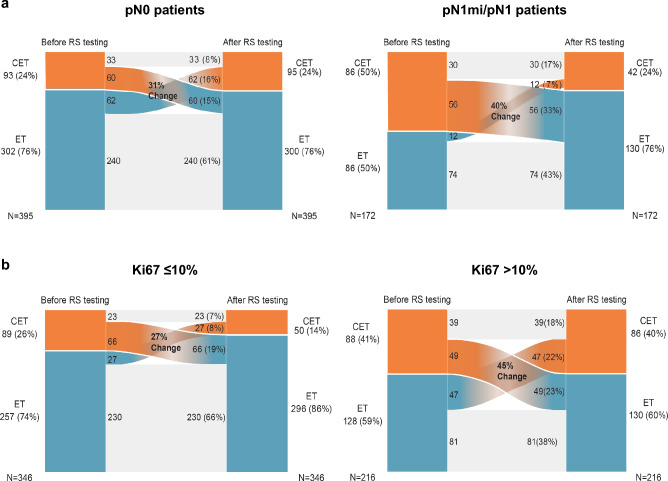
Results: The analysis included 567 patients (median age, 57 [range, 29-83] years; 70%/1%/29%/ with pN0/pN1mi/pN1 disease; 81% and 19% with RS results 0-25 and 26-100, respectively). The correlations between local and central Ki-67, local Ki-67, and the RS, and central Ki-67 and the RS results were weak (r = 0.35, r = 0.3, and r = 0.46, respectively), and discrepancies were noted in both directions (e.g., local Ki-67 was lower or higher than central Ki-67). After disclosing the RS, treatment recommendations changed for 190 patients (34%). Changes were observed in pN0 and pN1mi/pN1 patients and in patients with centrally determined Ki-67 ≤ 10% and > 10%. Treatment changes were aligned with RS results (adding chemotherapy for patients with higher RS results, omitting it for lower RS results), and their net result was 8% reduction in adjuvant chemotherapy use (from 32% pre-RS results to 24% post-RS results).
Conclusion: The Oncotype DX® assay is a tool for individualizing treatments that adds to classic treatment decision factors. The RS result and Ki-67 are not interchangeable, and Ki-67, as well as nodal status, should not be used as gatekeepers for testing eligibility, to avoid under and overtreatment.
Keywords: 21-gene assay; Adjuvant treatment; Breast cancer; Ki-67; Recurrence Score,; Registry.
© 2024. The Author(s).
Conflict of interest statement
Financial interests: C. Jackisch reports participating in advisory boards for Roche, AstraZeneca, Pfizer, Celgene, Lilly, and Exact Sciences; being a speaker and chairman for educational events for Roche, AstraZeneca, Pfizer, Celgene, Exact Sciences, Lilly, and Pierre-Fabré; and receiving research funding from Novartis, Exact Sciences, and Roche. M. Thill reports participating in advisory boards for Agendia, Amgen, AstraZeneca, Aurikamed, Becton/Dickinson, Biom ‘Up, ClearCut, Clovis, Daiichi Sankyo, Eisai, Exact Sciences, Gilead Science, Grünenthal, GSK, Lilly, MSD, Norgine, Neodynamics, Novartis, Onkowissen, Organon, Pfizer, pfm Medical, Pierre-Fabre, Roche, RTI Surgical, Seagen, Sirius Pintuition, and Sysmex; receiving manuscript support from Amgen, ClearCut, Clovis, pfm medical, Roche, and Servier; receiving travel support from Amgen, Art Tempi, AstraZeneca, Clearcut, Clovis, Connect Medica, Daiichi Sankyo, Eisai, Exact Sciences, Hexal, I-Med-Institute, Lilly, MCI, Medtronic, MSD, Norgine, Novartis, Pfizer, pfm Medical, Roche, RTI Surgical, and Seagen; congress support from Amgen, AstraZeneca, Celgene, Daiichi Sanyko, Hexal, Neodynamics, Novartis, Pfizer, and Roche; lecture honoraria from Amgen, Art Tempi, AstraZeneca, Clovis, Connect Medica, Eisai, Exact Sciences, Gilead Science, Hexal, I-Med-Institute, Jörg Eickeler, Lilly, MCI, Medtronic, MSD, Novartis, Omniamed, Onkowissen, Pfizer, pfm Medical, Roche, RTI Surgical, Seagen, Sysmex, Vifor, and Viatris; and trial funding from Endomag, and Exact Sciences. The remaining authors declare no competing financial or non-financial interests.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
