

APPaRENT 3: Asthma Patients' and Physicians' Perspectives on the Burden and Management of Asthma in Seven Countries
- PMID: 38874879
- PMCID: PMC11263244
- DOI: 10.1007/s12325-024-02900-2
APPaRENT 3: Asthma Patients' and Physicians' Perspectives on the Burden and Management of Asthma in Seven Countries
Abstract
Introduction: Asthma management is strongly dependent on physician and patient beliefs and perceptions about the disease and its long-term treatment. The APPaRENT 3 study was conducted to explore factors influencing treatment choice and to understand patients' and physicians' attitudes and perspectives on the use of controller inhalers in regular versus flexible dosing for asthma management.
Methods: This cross-sectional survey of patients with asthma and treating physicians was conducted in seven countries: Indonesia, Malaysia, Philippines, Thailand, Vietnam (patient survey only), Saudi Arabia, and the United Arab Emirates. Assessment was carried out through an online/face-to-face questionnaire, where patients' viewpoints were focused on their attitudes and beliefs about asthma and treatment adherence, whereas physicians' viewpoints were gathered on their attitudes and beliefs about asthma management, knowledge of and adherence to asthma treatment guidelines, and asthma treatment regimens.
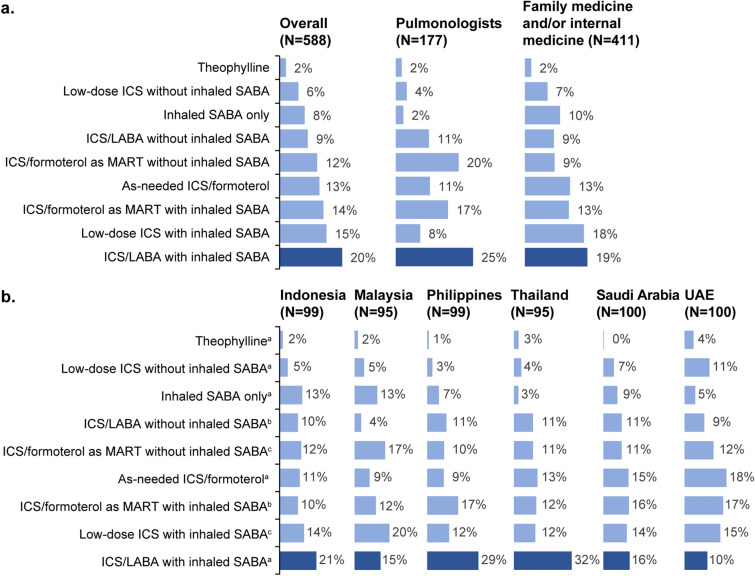
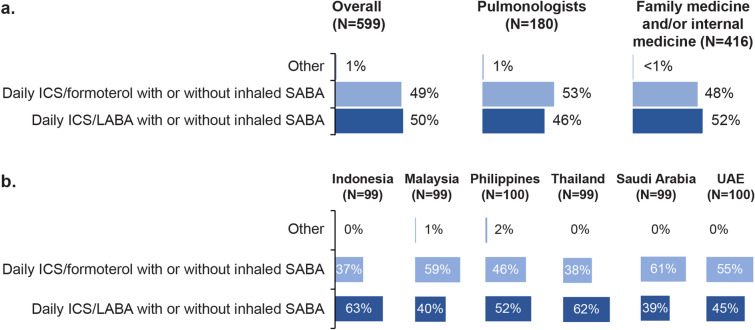
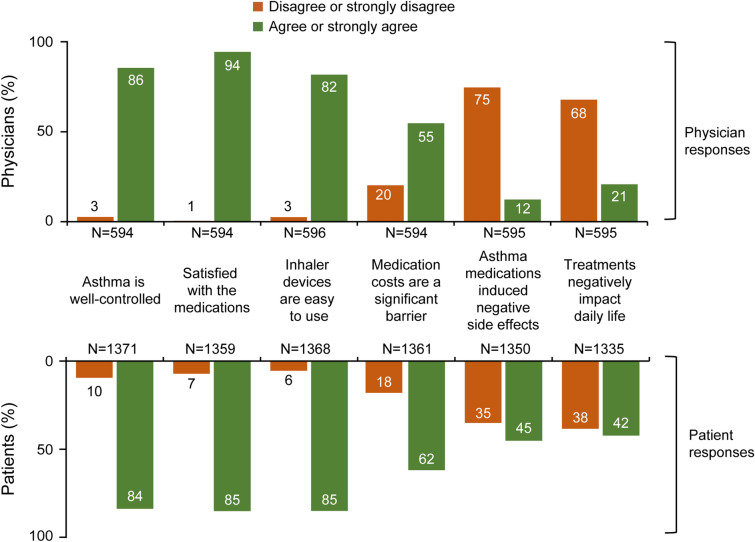
Results: Overall, 1400 patients (mean age, 34 years) and 599 physicians (mean age, 43 years) were included in the survey. Physicians similarly prioritised symptom control (39%) and exacerbation reduction (40%) in moderate asthma, whereas patients prioritised symptom control (41%) over exacerbation reduction (22%). Although both groups (physicians, 86%; patients, 84%) perceived asthma as well-controlled, poor management was evident based on Asthma Control Test (ACT) scores (mean, 15.7; standard deviation, 4.14; 82% had an ACT score < 20) and high symptom burden (39% reported nighttime awakenings or early mornings ≥ 2 nights/week). Most patients (76%) with moderate asthma were prescribed regular dosing, with the most common treatment being inhaled corticosteroid (ICS)/long-acting β2-agonist (LABA) with as-needed inhaled short-acting β2-agonist (SABA; 20%). Among patients on maintenance and reliever therapy, 93% of patients received a separate inhaled reliever.
Conclusions: Despite high symptom burden, patients overestimated their level of asthma control. Physicians prioritised controlling symptoms and reducing exacerbations as treatment goals for moderate asthma, often prescribing regular dosing with ICS/LABA with as-needed inhaled SABA.
Keywords: Asthma; Asthma control; Asthma exacerbation; Asthma regimen; Guideline adherence; Patient viewpoints; Physician perspectives.
Plain language summary
Managing asthma depends a lot on what doctors and patients think about the illness and its long-term treatment. This study looked into what influences treatment decisions and what patients and doctors think about using inhalers regularly or on an as-needed basis to manage asthma across seven countries (Indonesia, Malaysia, Philippines, Thailand, Vietnam [patient survey only], Saudi Arabia, and the United Arab Emirates). In this study, patients with asthma and doctors managing asthma completed an online/face-to-face questionnaire. The study aimed to understand what patients think about asthma and their treatment plan. Meanwhile, the doctors were asked what they think about managing asthma and how much they apply clinical guidelines for treating patients with asthma. Doctors believed it is equally important to control symptoms and prevent worsening of symptoms in patients with moderate asthma, while patients cared more about controlling symptoms than preventing worsening of symptoms. While doctors and patients both regarded asthma as well-controlled, many patients had low Asthma Control Test scores and experienced a lot of symptoms, suggesting that they are poor perceivers of asthma control. Most patients with moderate asthma were given regular treatment, usually with inhaled corticosteroid combined with long-acting β2-agonist along with as-needed short-acting β2-agonist as a reliever. Most patients who were prescribed the same inhaler for regular use and as a reliever also had a separate inhaler for quick relief of symptoms. This study shows the need for patients and doctors to have better conversations about asthma, its treatments, and what to expect from them.
© 2024. The Author(s).
Conflict of interest statement
Andrea Ban Yu-Lin received consulting fees from GSK, AstraZeneca, Boehringer Ingelheim, Menarini, Orient Pharma, and Pfizer and received payment or honoraria for lectures, presentations, speaker bureaus, manuscript writing, or educational events from GSK, AstraZeneca, Boehringer Ingelheim, Orient Pharma, Bayer, and Pfizer. Abhay Phansalkar is an employee of GSK and holds stocks/shares in GSK. Ashraf Alzaabi, Ahmad Izuanuddin Ismail, Orapan Poachanukoon, Muhammad Amin, and Thitiwat Sriprasart declared no competing interests. Bhumika Aggarwal and Gur Levy are employees of GSK and received support from GSK for the current manuscript. Farouz Rafih is an employee of GSK and does not hold stocks/shares in GSK. Gary Milligan, Laura Miriams, and Mark Silvey are employees of Adelphi Real World, which received funding to conduct the study and medical writing support for this manuscript. Mona Al-Ahmad received grants or contracts from Kuwait University and honoraria for lectures and advisory boards from GSK, AstraZeneca, and Sanofi. Mohamed Al-Moamary received consulting fees from Alhekma; received payment or honoraria for lectures, presentations, speaker bureaus, manuscript writing, or educational events from GSK, Novartis, AstraZeneca, and Abbott; and participated in a Data Safety Monitoring Board or Advisory Board for GSK. Maria Encarnita B. Limpin received honoraria for lectures on asthma from GSK, lectures on VTE from Corbridge, and lectures on COPD from Inova; she has been the past President of the Philippine College of Physicians & Philippine College of Chest Physicians, and Executive Director of Action on Smoking & Health, Philippines. Nguyen Van Tho received honoraria for lectures from GSK, AstraZeneca, Boehringer Ingelheim, and Novartis and received support for attending meetings from GSK, AstraZeneca, and Boehringer Ingelheim. Pham Thi Le Quyen received honoraria for lectures, presentations from GSK, AstraZeneca, Boehringer Ingelheim, Novartis, and Abbott. Riyad Allehebi received payment or honoraria for lectures, presentations, speaker bureaus, manuscript writing, or educational events from GSK, AstraZeneca, and Sanofi and received support from AstraZeneca, GSK, and Sanofi for attending meetings and/or travel. Steven Koenig received payment or honoraria for lectures, presentations, speaker bureaus, manuscript writing, or educational events from GSK. Triya Damayanti received payment or honoraria for lectures, presentations, speaker bureaus from GSK, AstraZeneca, Wellesta, and Zuelig and received support for attending meetings and/or travel from Zambon and GSK.
Figures
References
-
- Kementerian Kesehatan Republik Indonesia. Hasil Utama Riskesdas 2018. 2018. Available at: http://stikep-ppnijabar.ac.id/images/RISKESDAS_LAUNCHING_301018_edit2710.... Accessed: Mar 1, 2024.
-
- MaHTAS. Clinical practice guidelines. Management of asthma in adults. 2017. Available at: https://www.moh.gov.my/moh/resources/Penerbitan/CPG/Respiratory/CPG%20Ma.... Accessed: Jan 24, 2024.
-
- Varona LL, Alava HA, Abong JM, Castor MR, DeLeon JC, Kwong SL. Prevalence of asthma among Filipino adults based on the National Nutrition and Health Survey (NNHeS). Philipp J Intern Med. 2014;52:182–8.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
