

Population Pharmacokinetics of Cabozantinib in Metastatic Renal Cell Carcinoma Patients: Towards Drug Expenses Saving Regimens
- PMID: 38874883
- PMCID: PMC11222182
- DOI: 10.1007/s40262-024-01379-y
Population Pharmacokinetics of Cabozantinib in Metastatic Renal Cell Carcinoma Patients: Towards Drug Expenses Saving Regimens
Abstract
Introduction: Cabozantinib is one of the preferred treatment options in the latest metastatic renal cell carcinoma (mRCC) guidelines. Cabozantinib is also associated with high drug expenses irrespective of the used dose, because a flat-prizing model has been implemented. In addition, concomitant intake with a high-fat meal increases its bioavailability on average by 57%. Combined with the long terminal half-life of cabozantinib (99 h), this creates possibilities to extend the dosing interval to reduce drug expenses whilst maintaining equivalent exposure.
Objectives: The primary objective was to evaluate the population pharmacokinetic (POPPK) model of cabozantinib developed for its registration using real-world patients' therapeutic drug monitoring (TDM) data. The secondary objective was to design, simulate, and evaluate alternative dose regimens with the aim to reduce drug expenses whilst maintaining comparable exposure.
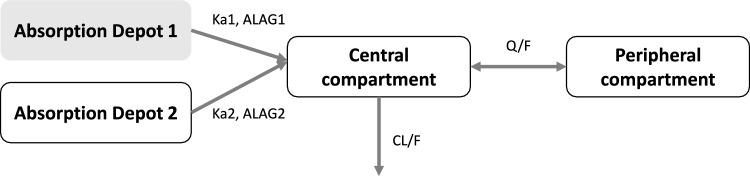
Methods: Retrospective TDM data from mRCC patients treated with cabozantinib were obtained. The data were evaluated using the published Food and Drug Administration (FDA) cabozantinib POPPK model, a two-compartment disposition model with a dual (fast and slow) lagged first-order absorption process derived from FDA registration documents, as a basis. Subsequently, simulations of alternative drug expenses saving regimens were evaluated.
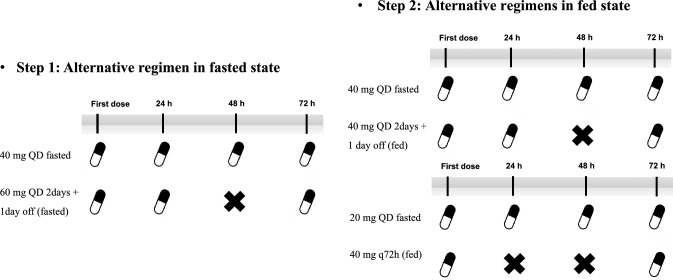
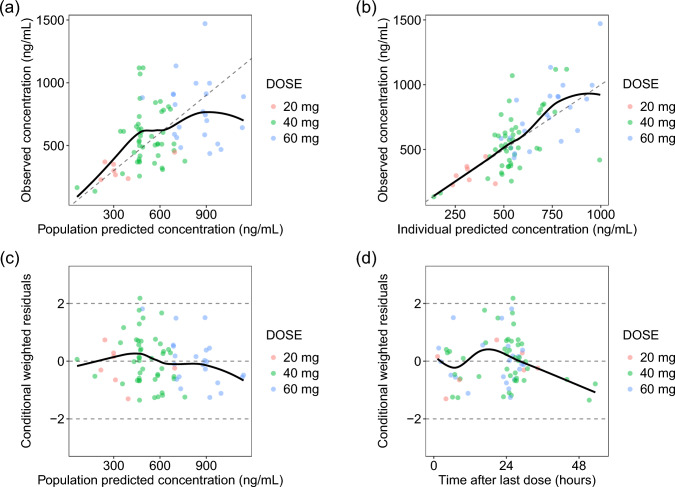
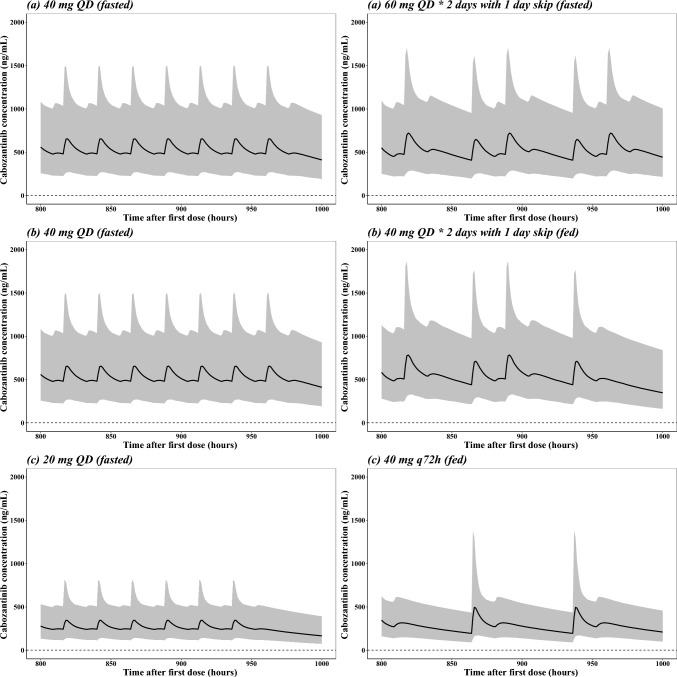
Results: Twenty-seven mRCC patients with 75 pharmacokinetic observations were included. Patients were treated for a median of 75 days with a median dose of 40 mg. Model evaluation results showed that the cabozantinib TDM concentrations were adequately predicted by the published FDA cabozantinib POPPK model, except for a slightly higher clearance (CL) of 3.11 L/h compared to the reported value (2.23 L/h). The simulation study indicated that an alternative dose regimen that consists of taking 60 mg of cabozantinib for 2 days and then skipping 1 day results in comparable average exposure when compared with a 40 mg daily dose, both without food interaction, while saving 33.3% of the total drug expenses per month. The food effect of a high-fat meal was also taken into account when simulating other alternative dose regimens; 40 mg every 72 h combined with a high-fat meal resulted in comparable exposure when compared with a 20 mg daily dose fasted, while saving 66.7% in drug expenses.
Conclusions: In this study, the optimized cabozantinib POPPK model resulted in adequate prediction of real-world cabozantinib pharmacokinetic data. Alternative dosing regimens with and without using known food interactions were proposed that resulted in potential strategies to significantly reduce cabozantinib drug expenses.
© 2024. The Author(s).
Conflict of interest statement
No disclosures are applicable for this work. None of the other authors have any conflicts to declare.
Figures
Similar articles
-
The Additional Costs per Month of Progression-Free Survival and Overall Survival: An Economic Model Comparing Everolimus with Cabozantinib, Nivolumab, and Axitinib for Second-Line Treatment of Metastatic Renal Cell Carcinoma.J Manag Care Spec Pharm. 2018 Apr;24(4):335-343. doi: 10.18553/jmcp.2018.24.4.335. J Manag Care Spec Pharm. 2018. PMID: 29578848 Free PMC article.
-
A population pharmacokinetic model of cabozantinib in healthy volunteers and patients with various cancer types.Cancer Chemother Pharmacol. 2018 Jun;81(6):1071-1082. doi: 10.1007/s00280-018-3581-0. Epub 2018 Apr 23. Cancer Chemother Pharmacol. 2018. PMID: 29687244 Free PMC article.
-
Exposure-response analyses of cabozantinib in patients with metastatic renal cell cancer.BMC Cancer. 2022 Mar 2;22(1):228. doi: 10.1186/s12885-022-09338-1. BMC Cancer. 2022. PMID: 35236333 Free PMC article.
-
Exposure-response modeling of cabozantinib in patients with renal cell carcinoma: Implications for patient care.Cancer Treat Rev. 2020 Sep;89:102062. doi: 10.1016/j.ctrv.2020.102062. Epub 2020 Jun 24. Cancer Treat Rev. 2020. PMID: 32659623 Review.
-
Clinical Pharmacokinetics and Pharmacodynamics of Cabozantinib.Clin Pharmacokinet. 2017 May;56(5):477-491. doi: 10.1007/s40262-016-0461-9. Clin Pharmacokinet. 2017. PMID: 27734291 Review.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
