

Quantitative Assessment of Lid Margin Vascularity Using Swept-Source Optical Coherence Tomography Angiography
- PMID: 38874976
- PMCID: PMC11182367
- DOI: 10.1167/tvst.13.6.6
Quantitative Assessment of Lid Margin Vascularity Using Swept-Source Optical Coherence Tomography Angiography
Abstract
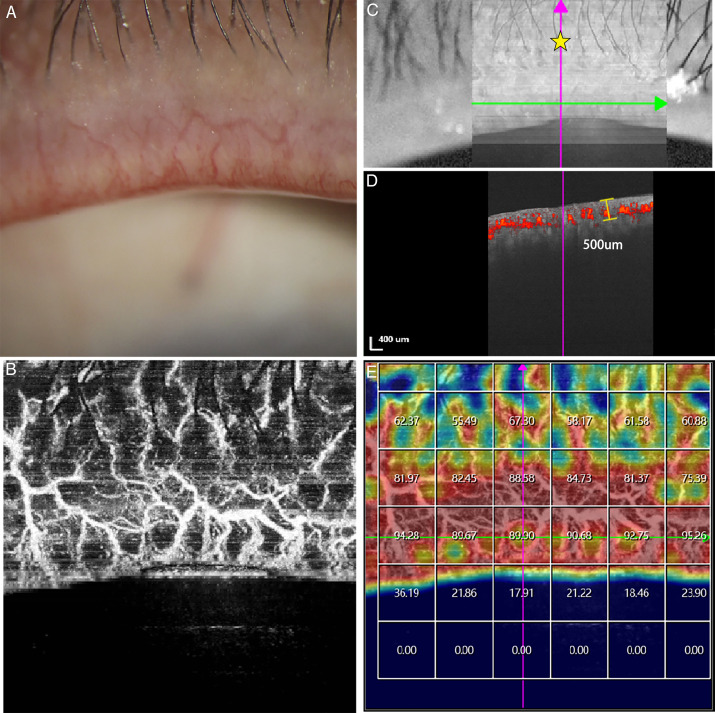
Purpose: To evaluate the ability of swept-source optical coherence tomography angiography (SS-OCTA) to assess lid margin vascularity.
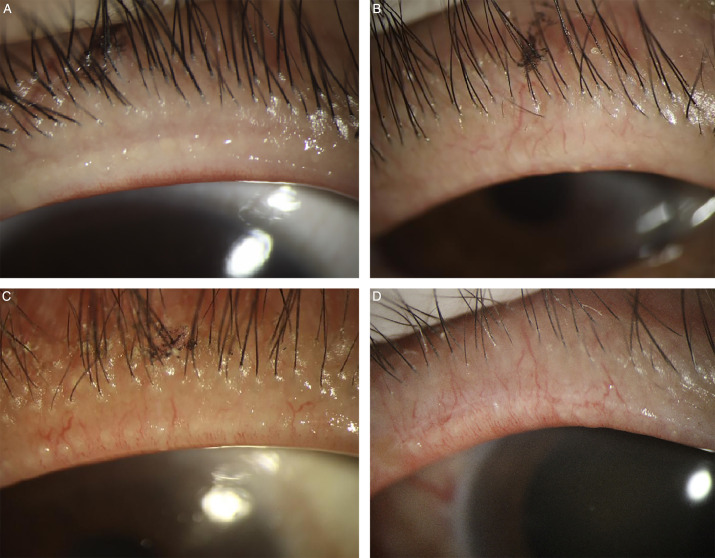
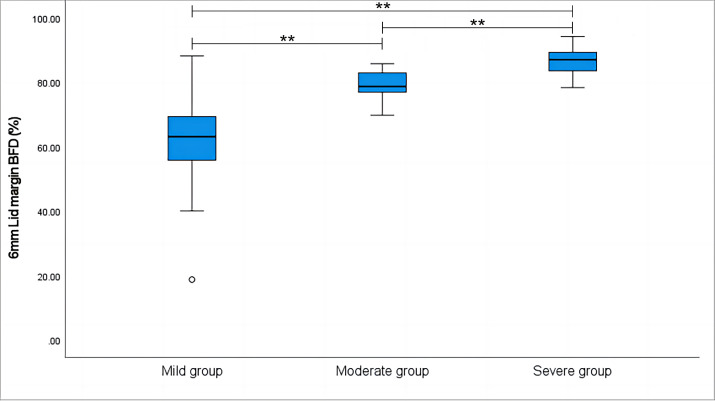
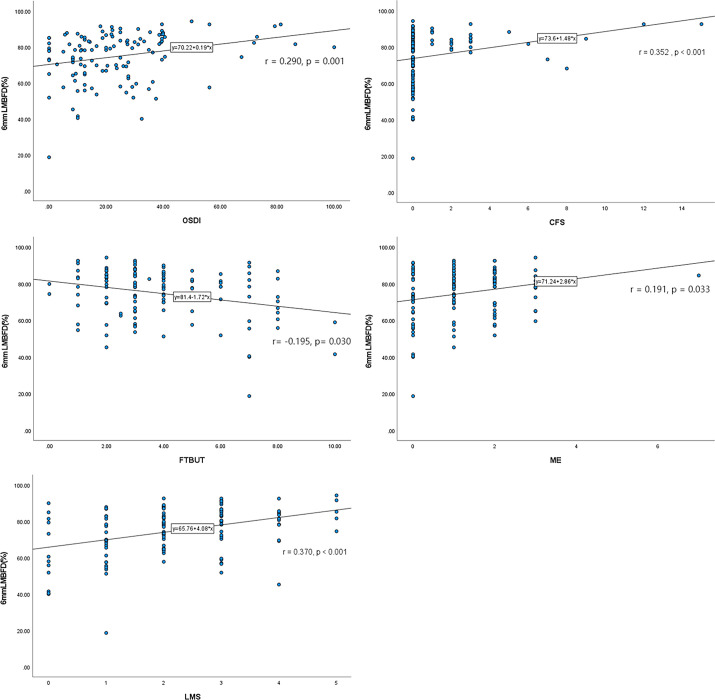
Methods: This prospective, cross-sectional trial enrolled 125 participants, including 15 control subjects and 110 meibomian gland dysfunction (MGD) patients. Lid margin blood flow density (LMBFD) was obtained using SS-OCTA. LMBFD was assessed for repeatability in 54 of 125 participants and for reproducibility in 23 of 125 participants. The efficacy of LMBFD was validated in the 125 participants, who were divided into mild (n = 46), moderate (n = 42), and severe groups (n = 37) according to the lid margin vascularity severity shown in the slit-lamp photographs. Correlations between LMBFD and MG-related parameters, such as ocular surface disease index (OSDI), fluorescein tear break-up time (FTBUT), cornea fluorescein staining (CFS), lid margin score (LMS), and meibomian gland expressibility (ME), were analyzed in all 125 participants.
Results: Repeatability and reproducibility coefficients were satisfactorily high in the scan mode with a scan area of 6 mm × 6 mm (intraclass correlation coefficient [ICC] repeatability = 0.905; ICC reproducibility = 0.986) and a scan area of 9 mm × 9 mm (ICC repeatability = 0.888; ICC reproducibility = 0.988). The LMBFD gradually increased in the mild, moderate, and severe groups (P < 0.001). LMBFD was significant correlated with OSDI (r = 0.290, P = 0.001), FTBUT (r = -0.195, P = 0.030), CFS (r = 0.352, P < 0.001), ME (r = 0.191, P = 0.033), and LMS (r = 0.370, P < 0.001).
Conclusions: LMBFD may be a noninvasive, repeatable, reproducible, and efficient index for the quantitative evaluation of eyelid margin vascularity in the future.
Translational relevance: We demonstrated that SS-OCTA has the potential to evaluate the eyelid margin vascularity in MGD patients and guide future treatment strategies in clinics.
Conflict of interest statement
Disclosure:
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
