

Seizure Assessment and Forecasting With Efficient Rapid-EEG: A Retrospective Multicenter Comparative Effectiveness Study
- PMID: 38875512
- PMCID: PMC12530332
- DOI: 10.1212/WNL.0000000000209621
Seizure Assessment and Forecasting With Efficient Rapid-EEG: A Retrospective Multicenter Comparative Effectiveness Study
Erratum in
-
Seizure Assessment and Forecasting With Efficient Rapid-EEG: A Retrospective Multicenter Comparative Effectiveness Study.Neurology. 2024 Nov 12;103(9):e209840. doi: 10.1212/WNL.0000000000209840. Epub 2024 Oct 14. Neurology. 2024. PMID: 39401404 No abstract available.
-
Correction to Author Disclosures.Neurology. 2024 Dec 24;103(12):e210123. doi: 10.1212/WNL.0000000000210123. Epub 2024 Nov 21. Neurology. 2024. PMID: 39571126 Free PMC article. No abstract available.
Abstract
Background and objectives: Approximately 30% of critically ill patients have seizures, and more than half of these seizures do not have an overt clinical correlate. EEG is needed to avoid missing seizures and prevent overtreatment with antiseizure medications. Conventional-EEG (cEEG) resources are logistically constrained and unable to meet their growing demand for seizure detection even in highly developed centers. Brief EEG screening with the validated 2HELPS2B algorithm was proposed as a method to triage cEEG resources, but it is hampered by cEEG requirements, primarily EEG technologists. Seizure risk-stratification using reduced time-to-application rapid response-EEG (rrEEG) systems (∼5 minutes) could be a solution. We assessed the noninferiority of the 2HELPS2B score on a 1-hour rrEEG compared to cEEG.
Methods: A multicenter retrospective EEG diagnostic accuracy study was conducted from October 1, 2021, to July 31, 2022. Chart and EEG review performed with consecutive sampling at 4 tertiary care centers, included records of patients ≥18 years old, from January 1, 2018, to June 20, 2022. Monte Carlo simulation power analysis yielded n = 500 rrEEG; for secondary outcomes n = 500 cEEG and propensity-score covariate matching was planned. Primary outcome, noninferiority of rrEEG for seizure risk prediction, was assessed per area under the receiver operator characteristic curve (AUC). Noninferiority margin (0.05) was based on the 2HELPS2B validation study.
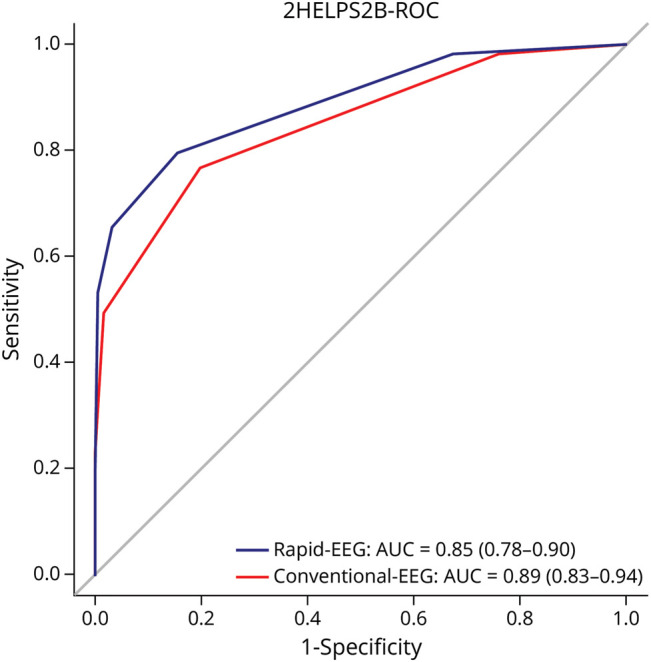
Results: A total of 240 rrEEG with follow-on cEEG were obtained. Median age was 64 (interquartile range 22); 42% were female. 2HELPS2B on a 1-hour rrEEG met noninferiority to cEEG (AUC 0.85, 95% CI 0.78-0.90, p = 0.001). Secondary endpoints of comparison with a matched contemporaneous cEEG showed no significant difference in AUC (0.89, 95% CI 0.83-0.94, p = 0.31); in false negative rate for the 2HELPS2B = 0 group (p = 1.0) rrEEG (0.021, 95% CI 0-0.062), cEEG (0.016, 95% CI 0-0.048); nor in survival analyses.
Discussion: 2HELPS2B on 1-hour rrEEG is noninferior to cEEG for seizure prediction. Patients with low-risk (2HELPS2B = 0) may be able to forgo prolonged cEEG, allowing for increased monitoring of at-risk patients.
Classification of evidence: This study provides Class II evidence that rrEEG is noninferior to cEEG in calculating the 2HELPS2B score to predict seizure risk.
Conflict of interest statement
L.J. Hirsch receives royalties from Wiley and Wolters Kluwer for co authoring and authoring a book and book chapters, respectively, receives consulting fees from Accure, Ceribell, Eisai, Marinus, Neurelis, Neuropace, Rafa Laboratories, and UCB, receives honoraria for organizing webinars for Neuropace, Natus, and UCB, and is co-chair, medical and scientific advisory board. All other authors report no relevant disclosures. Go to
Figures



References
-
- Claassen J, Taccone FS, Horn P, Holtkamp M, Stocchetti N, Oddo M; Neurointensive Care Section of the European Society of Intensive Care Medicine. Recommendations on the use of EEG monitoring in critically ill patients: consensus statement from the neurointensive care section of the ESICM. Intensive Care Med. 2013;39(8):1337-1351. doi: 10.1007/s00134-013-2938-4 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous