

MOSAIC: An Artificial Intelligence-Based Framework for Multimodal Analysis, Classification, and Personalized Prognostic Assessment in Rare Cancers
- PMID: 38875514
- PMCID: PMC11371092
- DOI: 10.1200/CCI.24.00008
MOSAIC: An Artificial Intelligence-Based Framework for Multimodal Analysis, Classification, and Personalized Prognostic Assessment in Rare Cancers
Abstract
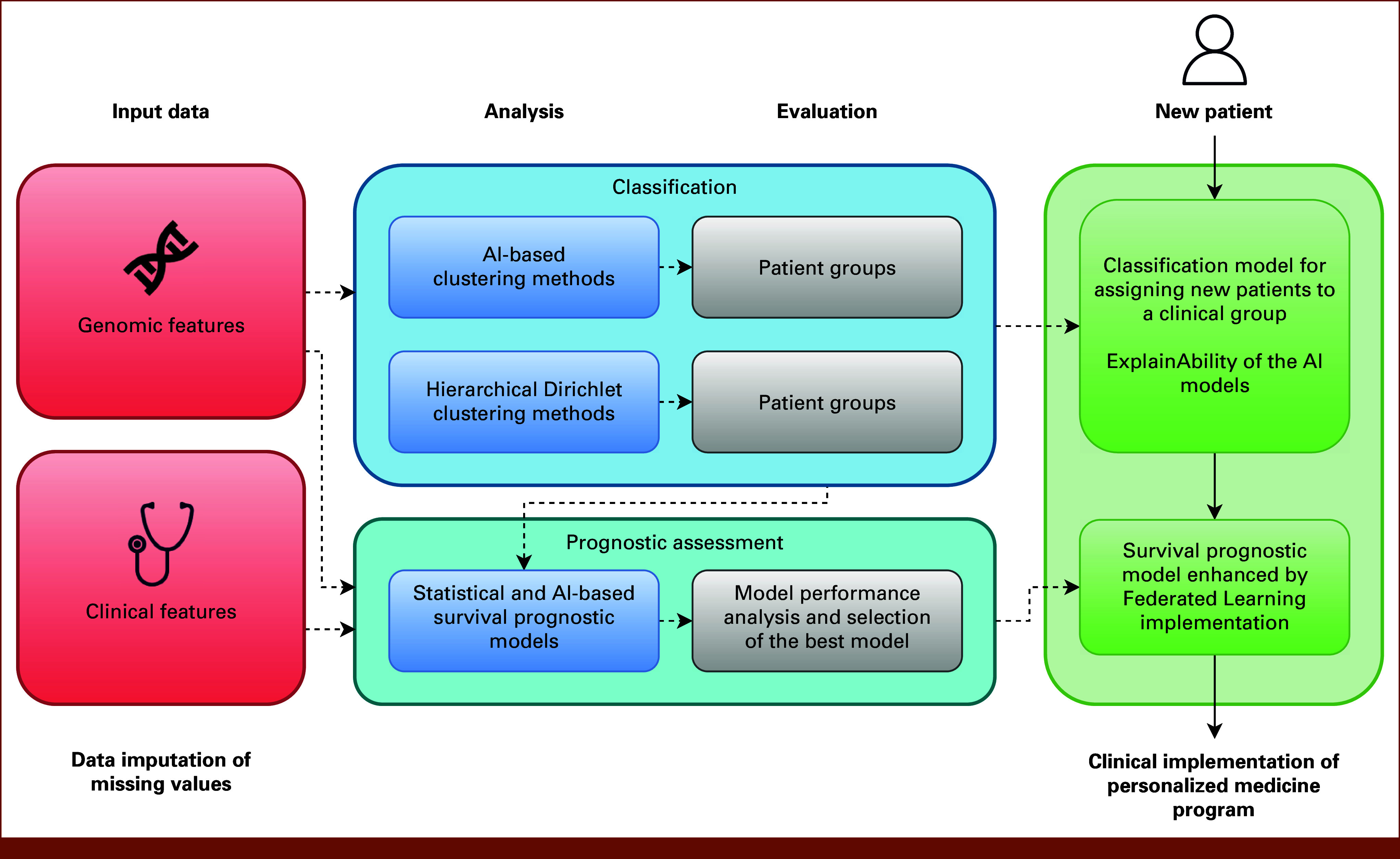
Purpose: Rare cancers constitute over 20% of human neoplasms, often affecting patients with unmet medical needs. The development of effective classification and prognostication systems is crucial to improve the decision-making process and drive innovative treatment strategies. We have created and implemented MOSAIC, an artificial intelligence (AI)-based framework designed for multimodal analysis, classification, and personalized prognostic assessment in rare cancers. Clinical validation was performed on myelodysplastic syndrome (MDS), a rare hematologic cancer with clinical and genomic heterogeneities.
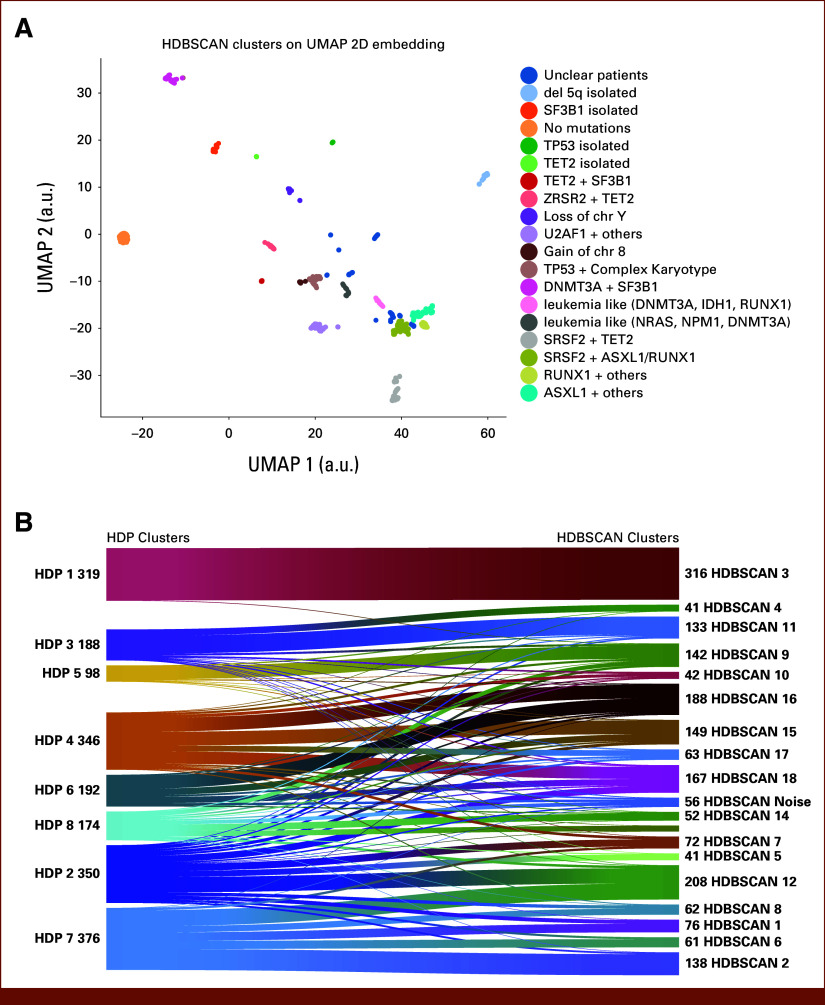
Methods: We analyzed 4,427 patients with MDS divided into training and validation cohorts. Deep learning methods were applied to integrate and impute clinical/genomic features. Clustering was performed by combining Uniform Manifold Approximation and Projection for Dimension Reduction + Hierarchical Density-Based Spatial Clustering of Applications with Noise (UMAP + HDBSCAN) methods, compared with the conventional Hierarchical Dirichlet Process (HDP). Linear and AI-based nonlinear approaches were compared for survival prediction. Explainable AI (Shapley Additive Explanations approach [SHAP]) and federated learning were used to improve the interpretation and the performance of the clinical models, integrating them into distributed infrastructure.
Results: UMAP + HDBSCAN clustering obtained a more granular patient stratification, achieving a higher average silhouette coefficient (0.16) with respect to HDP (0.01) and higher balanced accuracy in cluster classification by Random Forest (92.7% ± 1.3% and 85.8% ± 0.8%). AI methods for survival prediction outperform conventional statistical techniques and the reference prognostic tool for MDS. Nonlinear Gradient Boosting Survival stands in the internal (Concordance-Index [C-Index], 0.77; SD, 0.01) and external validation (C-Index, 0.74; SD, 0.02). SHAP analysis revealed that similar features drove patients' subgroups and outcomes in both training and validation cohorts. Federated implementation improved the accuracy of developed models.
Conclusion: MOSAIC provides an explainable and robust framework to optimize classification and prognostic assessment of rare cancers. AI-based approaches demonstrated superior accuracy in capturing genomic similarities and providing individual prognostic information compared with conventional statistical methods. Its federated implementation ensures broad clinical application, guaranteeing high performance and data protection.
Conflict of interest statement
The following represents disclosure information provided by authors of this manuscript. All relationships are considered compensated unless otherwise noted. Relationships are self-held unless noted. I = Immediate Family Member, Inst = My Institution. Relationships may not relate to the subject matter of this manuscript. For more information about ASCO's conflict of interest policy, please refer to
Open Payments is a public database containing information reported by companies about payments made to US-licensed physicians (
No other potential conflicts of interest were reported.
Figures



References
-
- Reference deleted.
-
- RARECARENet (information network on rare cancers). https://www.rarecarenet.eu/
-
- Gatta G, van der Zwan JM, Casali PG, et al. : Rare cancers are not so rare: The rare cancer burden in Europe. Eur J Cancer 47:2493-2511, 2011 - PubMed
-
- DeSantis CE, Kramer JL, Jemal A: The burden of rare cancers in the United States. CA Cancer J Clin 67:261-272, 2017 - PubMed
-
- Billingham L, Malottki K, Steven N: Research methods to change clinical practice for patients with rare cancers. Lancet Oncol 17:e70-e80, 2016 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
