

Seizure, Motor, and Cognitive Outcomes After Epilepsy Surgery for Patients With Sturge-Weber Syndrome: Results From a Multicenter Study
- PMID: 38875518
- PMCID: PMC11244739
- DOI: 10.1212/WNL.0000000000209525
Seizure, Motor, and Cognitive Outcomes After Epilepsy Surgery for Patients With Sturge-Weber Syndrome: Results From a Multicenter Study
Abstract
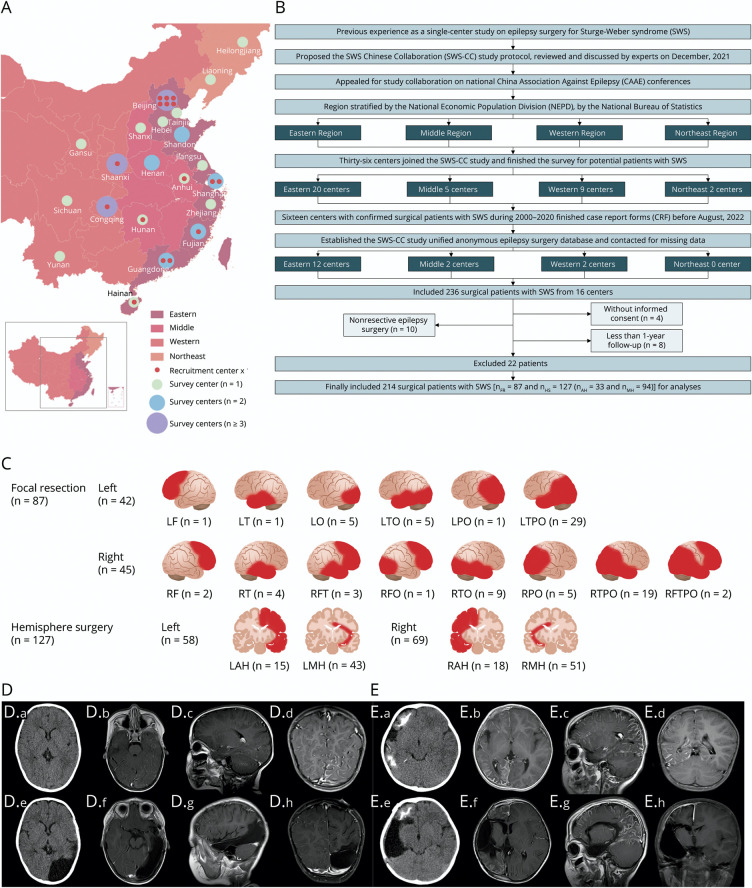
Background and objectives: Surgery is widely performed for refractory epilepsy in patients with Sturge-Weber syndrome (SWS), but reports on its effectiveness are limited. This study aimed to analyze seizure, motor, and cognitive outcomes of surgery in these patients and to identify factors associated with the outcomes.
Methods: This was a multicenter retrospective observational study using data from patients with SWS and refractory epilepsy who underwent epilepsy surgery between 2000 and 2020 at 16 centers throughout China. Longitudinal postoperative seizures were classified by Engel class, and Engel class I was regarded as seizure-free outcome. Functional (motor and cognitive) outcomes were evaluated using the SWS neurologic score, and improved or unchanged scores between baseline and follow-up were considered to have stable outcomes. Outcomes were analyzed using Kaplan-Meier analyses. Multivariate Cox regression was used to identify factors associated with outcomes.
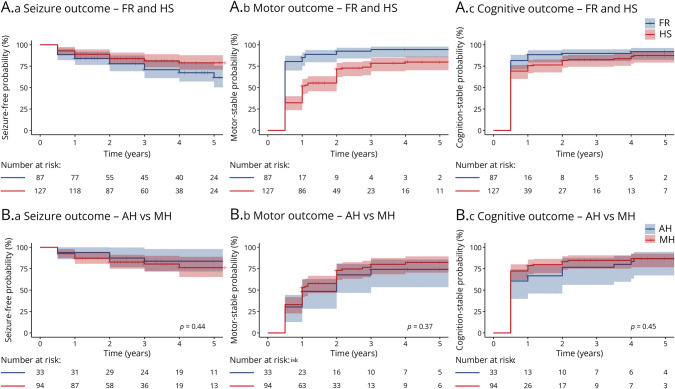
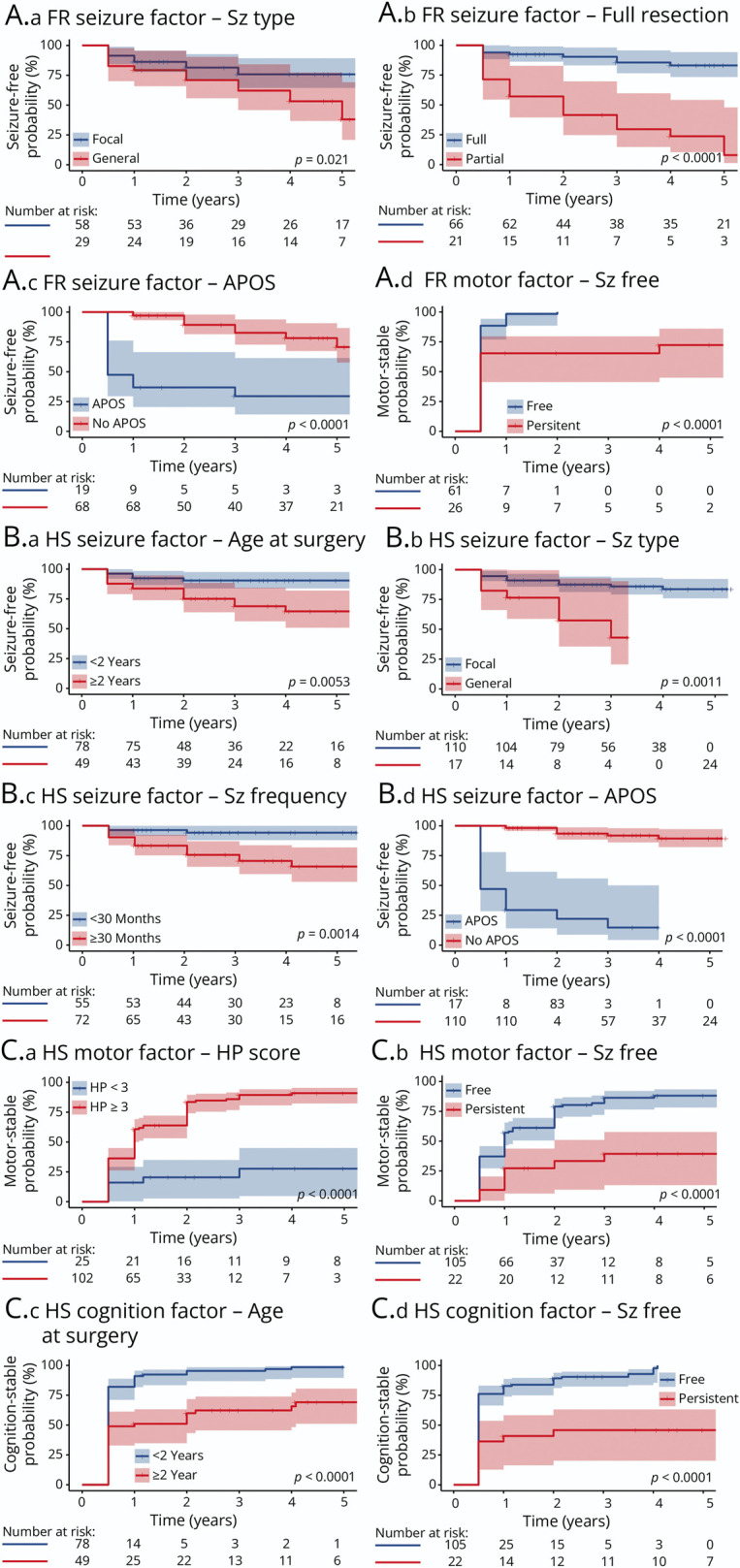
Results: A total of 214 patients with a median age of 2.0 (interquartile range 1.2-4.6) years underwent surgery (focal resection, FR [n = 87]; hemisphere surgery, HS [n = 127]) and completed a median of 3.5 (1.7-5.0) years of follow-up. The overall estimated probability for being seizure-free postoperatively at 1, 2, and 5 years was 86.9% (95% CI 82.5-91.6), 81.4% (95% CI 76.1-87.1), and 70.7% (95% CI 63.3-79.0), respectively. The overall estimated probability of being motor stable at the same time post operatively was 65.4% (95% CI 58.4-71.2), 80.2% (95% CI 73.8-85.0), and 85.7% (95% CI 79.5-90.1), respectively. The overall probability for being cognition stable at 1, 2, and 5 years was 80.8% (95% CI 74.8-85.5), 85.1% (95% CI 79.3-89.2), and 89.5% (95% CI 83.8-93.2), respectively. Both FR and HS were effective at ensuring seizure control. For different HS techniques, modified hemispherotomy had comparable outcomes but improved safety compared with anatomical hemispherectomy. Regarding FR, partial resection (adjusted hazard ratio [aHR] 11.50, 95% CI 4.44-29.76), acute postoperative seizure (APOS, within 30 days of surgery; aHR 10.33, 95% CI 3.94-27.12), and generalized seizure (aHR 3.09, 95% CI 1.37-6.94) were associated with seizure persistence. For HS, seizure persistence was associated with APOS (aHR 27.61, 9.92-76.89), generalized seizure (aHR 7.95, 2.74-23.05), seizure frequency ≥30 times/month (aHR 4.76, 1.27-17.87), and surgical age ≥2 years (aHR 3.78, 1.51-9.47); motor stability was associated with severe motor defects (aHR 5.23, 2.27-12.05) and postoperative seizure-free status (aHR 3.09, 1.49-6.45); and cognition stability was associated with postoperative seizure-free status (aHR 2.84, 1.39-5.78) and surgical age <2 years (aHR 1.76, 1.13-2.75).
Discussion: FR is a valid option for refractory epilepsy in patients with SWS and has similar outcomes to those of HS, with less morbidity associated with refractory epilepsy. Early surgical treatment (under the age of 2 years) leads to better outcomes after HS, but there is insufficient evidence that surgical age affects FR outcomes. These findings warrant future prospective multicenter cohorts with international cooperation and prolonged follow-up in better exploring more precise outcomes and developing prognostic predictive models.
Classification of evidence: This study provides Class IV evidence that in children with SWS and refractory seizures, surgical resection-focal, hemispherectomy, or modified hemispherotomy-leads to improved outcomes.
Conflict of interest statement
The authors report no relevant disclosures. Go to
Figures
Similar articles
-
Levetiracetam add-on for drug-resistant focal epilepsy: an updated Cochrane Review.Cochrane Database Syst Rev. 2012 Sep 12;2012(9):CD001901. doi: 10.1002/14651858.CD001901.pub2. Cochrane Database Syst Rev. 2012. PMID: 22972056 Free PMC article.
-
Epilepsy surgery in Sturge-Weber syndrome with unilateral or bilateral asymmetric brain involvement: Boston Children's Hospital experience.Epilepsia. 2025 Jul;66(7):2198-2212. doi: 10.1111/epi.18387. Epub 2025 Mar 24. Epilepsia. 2025. PMID: 40126015
-
Prognosis of adults and children following a first unprovoked seizure.Cochrane Database Syst Rev. 2023 Jan 23;1(1):CD013847. doi: 10.1002/14651858.CD013847.pub2. Cochrane Database Syst Rev. 2023. PMID: 36688481 Free PMC article.
-
Surgery for epilepsy.Cochrane Database Syst Rev. 2015 Jul 1;(7):CD010541. doi: 10.1002/14651858.CD010541.pub2. Cochrane Database Syst Rev. 2015. Update in: Cochrane Database Syst Rev. 2019 Jun 25;6:CD010541. doi: 10.1002/14651858.CD010541.pub3. PMID: 26130264 Updated.
-
Yoga for epilepsy.Cochrane Database Syst Rev. 2017 Oct 5;10(10):CD001524. doi: 10.1002/14651858.CD001524.pub3. Cochrane Database Syst Rev. 2017. PMID: 28982217 Free PMC article.
Cited by
-
Sturge-Weber Syndrome: A Narrative Review of Clinical Presentation and Updates on Management.J Clin Med. 2025 Mar 22;14(7):2182. doi: 10.3390/jcm14072182. J Clin Med. 2025. PMID: 40217631 Free PMC article. Review.
-
Hemispherotomy for drug-resistant epilepsy in bilateral Sturge-Weber syndrome: illustrative cases.J Neurosurg Case Lessons. 2025 Aug 4;10(5):CASE25125. doi: 10.3171/CASE25125. Print 2025 Aug 4. J Neurosurg Case Lessons. 2025. PMID: 40759056 Free PMC article.
-
Deep brain stimulation surgical timing, outcomes, and prognostic factors in patients with Parkinson's disease: A Chinese retrospective multicenter cohort study.PLoS Med. 2025 Aug 1;22(8):e1004670. doi: 10.1371/journal.pmed.1004670. eCollection 2025 Aug. PLoS Med. 2025. PMID: 40749017 Free PMC article.
-
Transcriptomic Profiling Unveils EDN3+ Meningeal Fibroblasts as Key Players in Sturge-Weber Syndrome Pathogenesis.Adv Sci (Weinh). 2025 May;12(17):e2408888. doi: 10.1002/advs.202408888. Epub 2025 Feb 8. Adv Sci (Weinh). 2025. PMID: 39921427 Free PMC article.
-
New Trigger for Stroke-like Episode in Sturge-Weber Syndrome: A Case Report.Children (Basel). 2025 Apr 30;12(5):589. doi: 10.3390/children12050589. Children (Basel). 2025. PMID: 40426769 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials