

Determinants of Intravenous Infusion Longevity and Infusion Failure via a Nonlinear Model Analysis of Smart Pump Event Logs: Retrospective Study
- PMID: 38875535
- PMCID: PMC11041480
- DOI: 10.2196/48628
Determinants of Intravenous Infusion Longevity and Infusion Failure via a Nonlinear Model Analysis of Smart Pump Event Logs: Retrospective Study
Abstract
Background: Infusion failure may have severe consequences for patients receiving critical, short-half-life infusions. Continued interruptions to infusions can lead to subtherapeutic therapy.
Objective: This study aims to identify and rank determinants of the longevity of continuous infusions administered through syringe drivers, using nonlinear predictive models. Additionally, this study aims to evaluate key factors influencing infusion longevity and develop and test a model for predicting the likelihood of achieving successful infusion longevity.
Methods: Data were extracted from the event logs of smart pumps containing information on care profiles, medication types and concentrations, occlusion alarm settings, and the final infusion cessation cause. These data were then used to fit 5 nonlinear models and evaluate the best explanatory model.
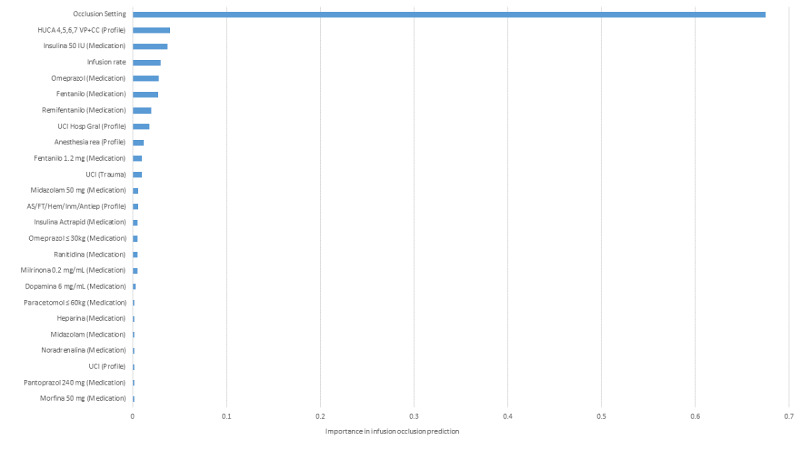
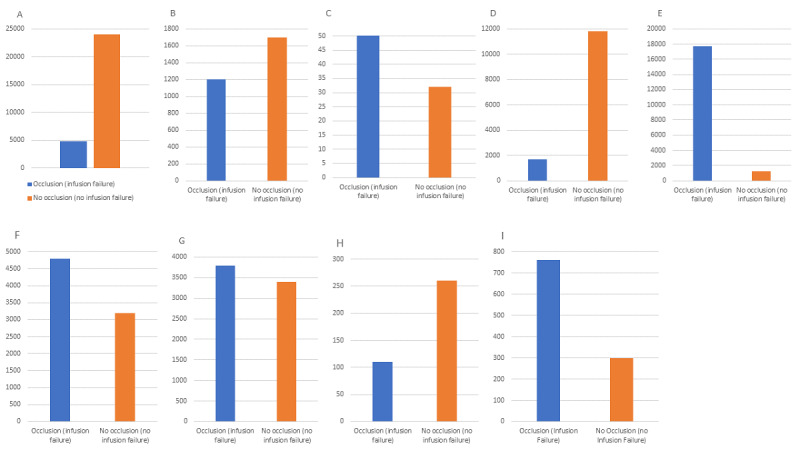
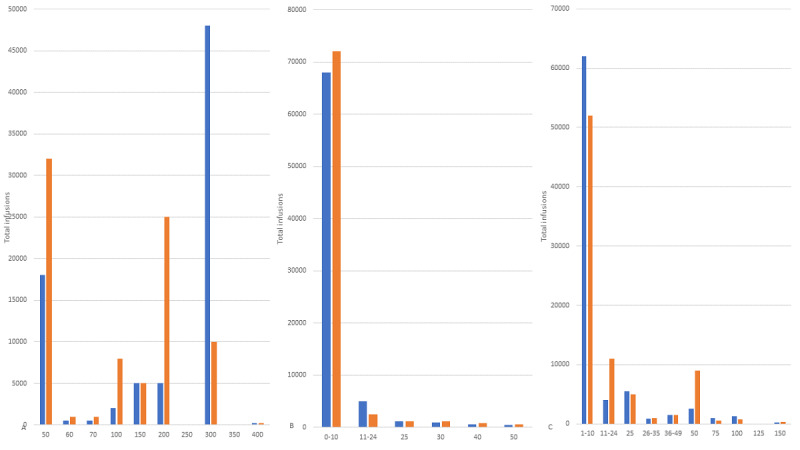
Results: Random forest was the best-fit predictor, with an F1-score of 80.42, compared to 5 other models (mean F1-score 75.06; range 67.48-79.63). When applied to infusion data in an individual syringe driver data set, the predictor model found that the final medication concentration and medication type were of less significance to infusion longevity compared to the rate and care unit. For low-rate infusions, rates ranging from 2 to 2.8 mL/hr performed best for achieving a balance between infusion longevity and fluid load per infusion, with an occlusion versus no-occlusion ratio of 0.553. Rates between 0.8 and 1.2 mL/hr exhibited the poorest performance with a ratio of 1.604. Higher rates, up to 4 mL/hr, performed better in terms of occlusion versus no-occlusion ratios.
Conclusions: This study provides clinicians with insights into the specific types of infusion that warrant more intense observation or proactive management of intravenous access; additionally, it can offer valuable information regarding the average duration of uninterrupted infusions that can be expected in these care areas. Optimizing rate settings to improve infusion longevity for continuous infusions, achieved through compounding to create customized concentrations for individual patients, may be possible in light of the study's outcomes. The study also highlights the potential of machine learning nonlinear models in predicting outcomes and life spans of specific therapies delivered via medical devices.
Keywords: AI; alarm fatigue; artificial intelligence; event log; health device; infusion; intensive care; intensive care units; intravenous; intravenous infusion; log data; machine learning; medical device; neonatal; nonlinear model; predict; prediction; prediction model; predictive; predictive model; smart device; smart pump; therapy; vascular access device.
©Arash Kia, James Waterson, Norma Bargary, Stuart Rolt, Kevin Burke, Jeremy Robertson, Samuel Garcia, Alessio Benavoli, David Bergström. Originally published in JMIR AI (https://ai.jmir.org), 13.09.2023.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures

Similar articles
-
Types and Frequency of Infusion Pump Alarms and Infusion-Interruption to Infusion-Recovery Times for Critical Short Half-Life Infusions: Retrospective Data Analysis.JMIR Hum Factors. 2019 Aug 12;6(3):e14123. doi: 10.2196/14123. JMIR Hum Factors. 2019. PMID: 31407667 Free PMC article.
-
Analysis of event logs from syringe pumps: a retrospective pilot study to assess possible effects of syringe pumps on safety in a university hospital critical care unit in Germany.Drug Saf. 2012 Jul 1;35(7):563-74. doi: 10.2165/11597350-000000000-00000. Drug Saf. 2012. PMID: 22671864
-
Dose error reduction software in medication safety risk management - optimising the smart infusion pump dosing limits in neonatal intensive care unit prior to implementation.BMC Pediatr. 2022 Mar 8;22(1):118. doi: 10.1186/s12887-022-03183-8. BMC Pediatr. 2022. PMID: 35255846 Free PMC article.
-
Smart syringe pumps for drug infusion during dental intravenous sedation.J Dent Anesth Pain Med. 2016 Sep;16(3):165-173. doi: 10.17245/jdapm.2016.16.3.165. Epub 2016 Sep 30. J Dent Anesth Pain Med. 2016. PMID: 28884149 Free PMC article. Review.
-
Intravenous Smart Pumps: Usability Issues, Intravenous Medication Administration Error, and Patient Safety.Crit Care Nurs Clin North Am. 2018 Jun;30(2):215-224. doi: 10.1016/j.cnc.2018.02.004. Epub 2018 Apr 7. Crit Care Nurs Clin North Am. 2018. PMID: 29724440 Review.
References
-
- Chaplin S. National Patient Safety Agency report: patient safety in the NHS. Prescriber. 2006 Apr 05;17(7):52–54. doi: 10.1002/psb.361. - DOI
-
- Waterson J, Bedner A. Types and frequency of infusion pump alarms and infusion-interruption to infusion-recovery times for critical short half-life infusions: retrospective data analysis. JMIR Hum Factors. 2019 Aug 12;6(3):e14123. doi: 10.2196/14123. https://humanfactors.jmir.org/2019/3/e14123/ v6i3e14123 - DOI - PMC - PubMed
-
- Krukas A, Franklin E, Bonk C, Howe J, Dixit R, Adams K, Krevat S, Jones R, Ratwani R. Identifying safety hazards associated with intravenous vancomycin through the analysis of patient safety event reports. PatientSaf. 2020 Mar 17;:31–47. doi: 10.33940/data/2020.3.3. - DOI
-
- Cho O, Kim H, Lee Y, Cho I. Clinical alarms in intensive care units: perceived obstacles of alarm management and alarm fatigue in nurses. Healthc Inform Res. 2016 Jan;22(1):46–53. doi: 10.4258/hir.2016.22.1.46. https://europepmc.org/abstract/MED/26893950 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
