

Predicting Patient Mortality for Earlier Palliative Care Identification in Medicare Advantage Plans: Features of a Machine Learning Model
- PMID: 38875557
- PMCID: PMC11041411
- DOI: 10.2196/42253
Predicting Patient Mortality for Earlier Palliative Care Identification in Medicare Advantage Plans: Features of a Machine Learning Model
Abstract
Background: Machine learning (ML) can offer greater precision and sensitivity in predicting Medicare patient end of life and potential need for palliative services compared to provider recommendations alone. However, earlier ML research on older community dwelling Medicare beneficiaries has provided insufficient exploration of key model feature impacts and the role of the social determinants of health.
Objective: This study describes the development of a binary classification ML model predicting 1-year mortality among Medicare Advantage plan members aged ≥65 years (N=318,774) and further examines the top features of the predictive model.
Methods: A light gradient-boosted trees model configuration was selected based on 5-fold cross-validation. The model was trained with 80% of cases (n=255,020) using randomized feature generation periods, with 20% (n=63,754) reserved as a holdout for validation. The final algorithm used 907 feature inputs extracted primarily from claims and administrative data capturing patient diagnoses, service utilization, demographics, and census tract-based social determinants index measures.
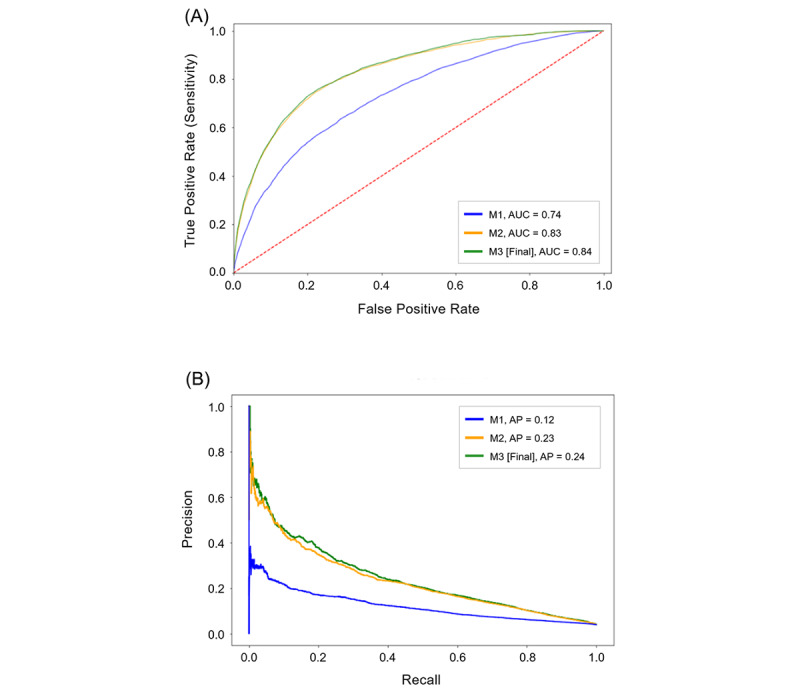
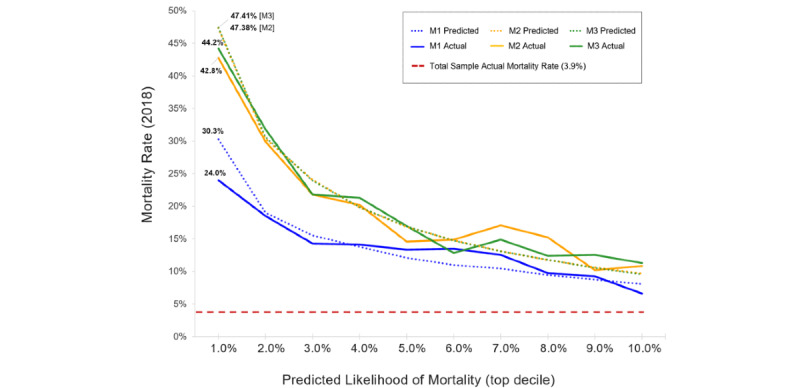
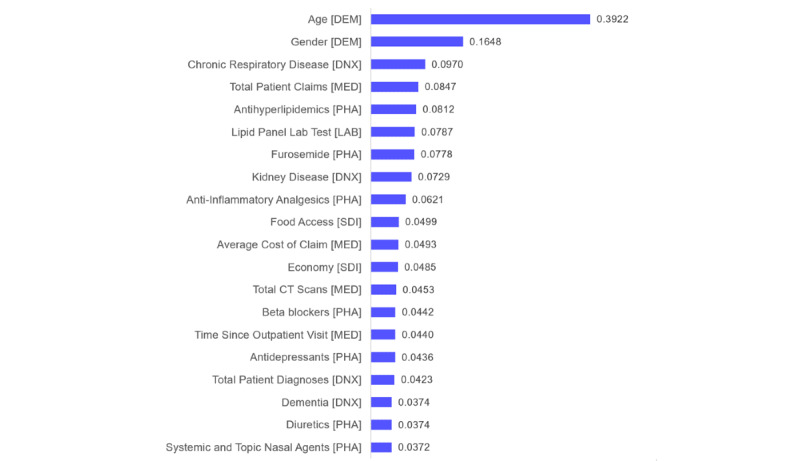
Results: The total sample had an actual mortality prevalence of 3.9% in the 2018 outcome period. The final model correctly predicted 44.2% of patient expirations among the top 1% of highest risk members (AUC=0.84; 95% CI 0.83-0.85) versus 24.0% predicted by the model iteration using only age, gender, and select high-risk utilization features (AUC=0.74; 95% CI 0.73-0.74). The most important algorithm features included patient demographics, diagnoses, pharmacy utilization, mean costs, and certain social determinants of health.
Conclusions: The final ML model better predicts Medicare Advantage member end of life using a variety of routinely collected data and supports earlier patient identification for palliative care.
Keywords: Medicare; Medicare Advantage; algorithm; machine learning; mortality; older adult; palliative; palliative care; predict; social determinants.
©Anne Bowers, Chelsea Drake, Alexi E Makarkin, Robert Monzyk, Biswajit Maity, Andrew Telle. Originally published in JMIR AI (https://ai.jmir.org), 20.02.2023.
Conflict of interest statement
Conflicts of Interest: AB, CD, AEM, RM, and AT are employees of the organization that requested and funded the study (Cigna/Evernorth). BM is a contracted employee of the same organization. The authors have no further interests to declare.
Figures
Similar articles
-
Can Predictive Modeling Tools Identify Patients at High Risk of Prolonged Opioid Use After ACL Reconstruction?Clin Orthop Relat Res. 2020 Jul;478(7):0-1618. doi: 10.1097/CORR.0000000000001251. Clin Orthop Relat Res. 2020. PMID: 32282466 Free PMC article.
-
Economic burden in direct costs of concomitant chronic obstructive pulmonary disease and asthma in a Medicare Advantage population.J Manag Care Pharm. 2008 Mar;14(2):176-85. doi: 10.18553/jmcp.2008.14.2.176. J Manag Care Pharm. 2008. PMID: 18331119 Free PMC article.
-
Development and validation of 15-month mortality prediction models: a retrospective observational comparison of machine-learning techniques in a national sample of Medicare recipients.BMJ Open. 2019 Jul 16;9(7):e022935. doi: 10.1136/bmjopen-2018-022935. BMJ Open. 2019. PMID: 31315852 Free PMC article.
-
Comparison of Machine Learning Methods With Traditional Models for Use of Administrative Claims With Electronic Medical Records to Predict Heart Failure Outcomes.JAMA Netw Open. 2020 Jan 3;3(1):e1918962. doi: 10.1001/jamanetworkopen.2019.18962. JAMA Netw Open. 2020. PMID: 31922560 Free PMC article.
-
Association between health system specialty pharmacy use and health care costs among national sample of Medicare Advantage beneficiaries.J Manag Care Spec Pharm. 2022 Feb;28(2):244-254. doi: 10.18553/jmcp.2022.28.2.244. J Manag Care Spec Pharm. 2022. PMID: 35098745 Free PMC article.
Cited by
-
Ethical Challenges and Opportunities of AI in End-of-Life Palliative Care: Integrative Review.Interact J Med Res. 2025 May 14;14:e73517. doi: 10.2196/73517. Interact J Med Res. 2025. PMID: 40302210 Free PMC article. Review.
References
-
- March 2021 Report to the Congress: Medicare Payment Policy. Medicare Payment Advisory Commission. 2021. [2023-01-06]. https://www.medpac.gov/document/march-2021-report-to-the-congress-medica...
-
- May P, Tysinger B, Morrison RS, Jacobson M. Advancing the economics of palliative care: The value to individuals and families, organizations, and society. USC Schaeffer Center for Health Policy & Economics. 2021. Aug 5, [2023-01-06]. https://healthpolicy.usc.edu/research/advancing-the-economics-of-palliat...
-
- Bevins J, Bhulani N, Goksu SY, Sanford NN, Gao A, Ahn C, Paulk ME, Terauchi S, Pruitt SL, Tavakkoli A, Rhodes RL, Kazmi SMA, Beg MS. Early palliative care is associated with reduced emergency department utilization in pancreatic cancer. Am J Clin Oncol. 2021 May 01;44(5):181–186. doi: 10.1097/COC.0000000000000802.00000421-202105000-00002 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
