

Machine Learning for the Prediction of Procedural Case Durations Developed Using a Large Multicenter Database: Algorithm Development and Validation Study
- PMID: 38875567
- PMCID: PMC11041482
- DOI: 10.2196/44909
Machine Learning for the Prediction of Procedural Case Durations Developed Using a Large Multicenter Database: Algorithm Development and Validation Study
Abstract
Background: Accurate projections of procedural case durations are complex but critical to the planning of perioperative staffing, operating room resources, and patient communication. Nonlinear prediction models using machine learning methods may provide opportunities for hospitals to improve upon current estimates of procedure duration.
Objective: The aim of this study was to determine whether a machine learning algorithm scalable across multiple centers could make estimations of case duration within a tolerance limit because there are substantial resources required for operating room functioning that relate to case duration.
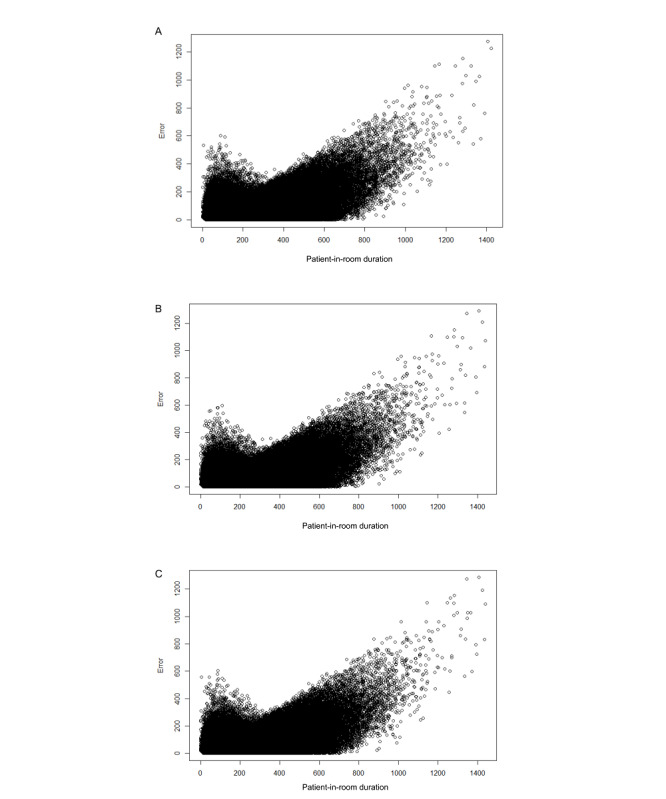
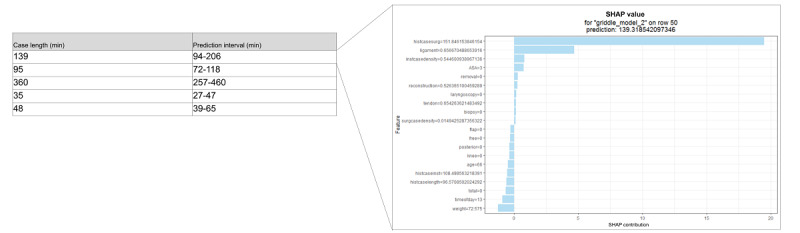
Methods: Deep learning, gradient boosting, and ensemble machine learning models were generated using perioperative data available at 3 distinct time points: the time of scheduling, the time of patient arrival to the operating or procedure room (primary model), and the time of surgical incision or procedure start. The primary outcome was procedure duration, defined by the time between the arrival and the departure of the patient from the procedure room. Model performance was assessed by mean absolute error (MAE), the proportion of predictions falling within 20% of the actual duration, and other standard metrics. Performance was compared with a baseline method of historical means within a linear regression model. Model features driving predictions were assessed using Shapley additive explanations values and permutation feature importance.
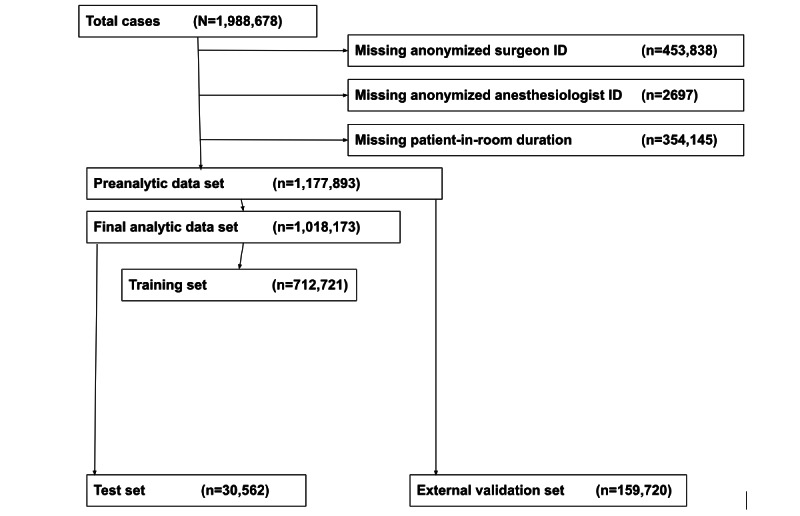
Results: A total of 1,177,893 procedures from 13 academic and private hospitals between 2016 and 2019 were used. Across all procedures, the median procedure duration was 94 (IQR 50-167) minutes. In estimating the procedure duration, the gradient boosting machine was the best-performing model, demonstrating an MAE of 34 (SD 47) minutes, with 46% of the predictions falling within 20% of the actual duration in the test data set. This represented a statistically and clinically significant improvement in predictions compared with a baseline linear regression model (MAE 43 min; P<.001; 39% of the predictions falling within 20% of the actual duration). The most important features in model training were historical procedure duration by surgeon, the word "free" within the procedure text, and the time of day.
Conclusions: Nonlinear models using machine learning techniques may be used to generate high-performing, automatable, explainable, and scalable prediction models for procedure duration.
Keywords: AI; OR management; algorithm development; artificial intelligence; machine learning; medical informatics; operating room; patient communication; perioperative; prediction model; surgical procedure; validation.
©Samir Kendale, Andrew Bishara, Michael Burns, Stuart Solomon, Matthew Corriere, Michael Mathis. Originally published in JMIR AI (https://ai.jmir.org), 08.09.2023.
Conflict of interest statement
Conflicts of Interest: AB is a co-founder of Bezel Health, a company building software to measure and improve healthcare quality interventions. SS is a co-founder of Orchestra Health Inc, a digital health startup company improving care transitions. This is unrelated to the work in this study.
Figures

References
-
- Edelman ER, van Kuijk SM, Hamaekers AE, de Korte MJ, van Merode GG, Buhre WF. Improving the prediction of total surgical procedure time using linear regression modeling. Front Med (Lausanne) 2017 Jun 19;4:85. doi: 10.3389/fmed.2017.00085. https://europepmc.org/abstract/MED/28674693 - DOI - PMC - PubMed
