

Cost-effectiveness of interventions for HIV/AIDS, malaria, syphilis, and tuberculosis in 128 countries: a meta-regression analysis
- PMID: 38876762
- PMCID: PMC11194165
- DOI: 10.1016/S2214-109X(24)00181-5
Cost-effectiveness of interventions for HIV/AIDS, malaria, syphilis, and tuberculosis in 128 countries: a meta-regression analysis
Abstract
Background: Cost-effectiveness analyses have been conducted for many interventions for HIV/AIDS, malaria, syphilis, and tuberculosis, but they have not been conducted for all interventions that are currently recommended in all countries. To support national decision makers in the effective allocation of resources, we conducted a meta-regression analysis of published incremental cost-effectiveness ratios (ICERs) for interventions for these causes, and predicted ICERs for 14 recommended interventions for Global Fund-eligible countries.
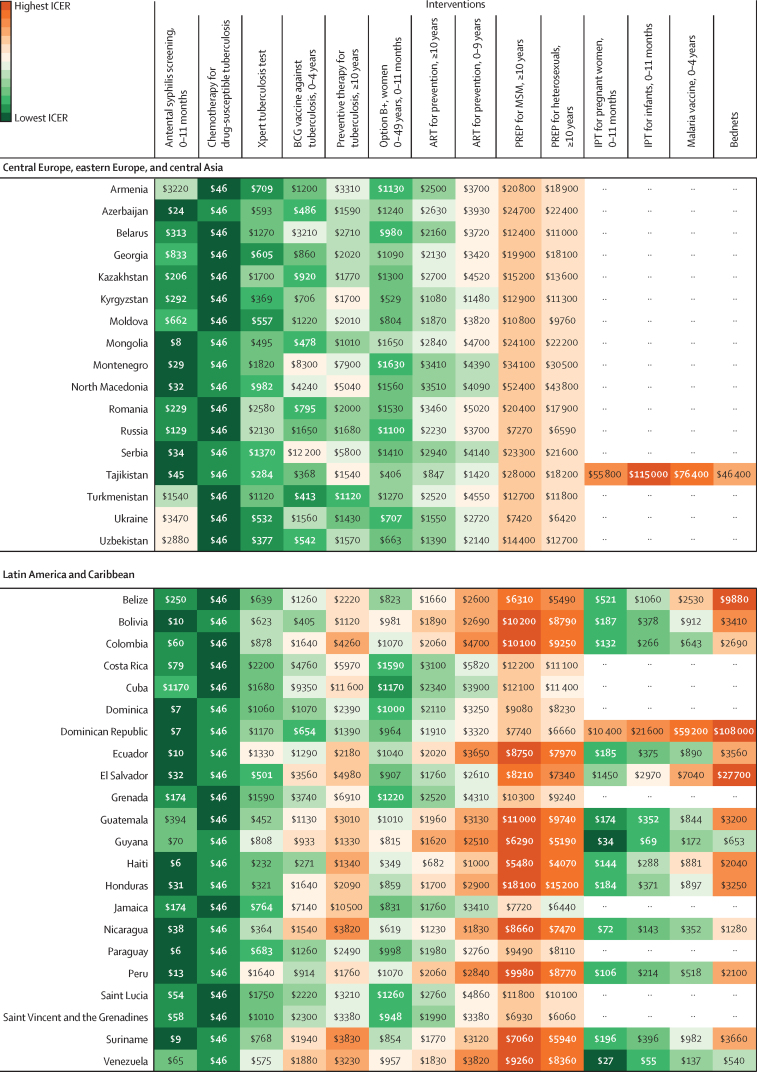
Methods: In the meta-regression analysis, we used data from the Tufts University Center for the Evaluation of Value and Risk in Health (Boston, MA, USA) Cost-Effectiveness Registries (the CEA Registry beginning in 1976 and the Global Health CEA registry beginning in 1995) up to Jan 1, 2018. To create analysis files, we standardised and mapped the data, extracted additional data from published articles, and added variables from the Global Burden of Diseases, Injuries, and Risk Factors Study (GBD). Then we selected ratios for interventions with a minimum of two published articles and three published ICERs that mapped to one of five GBD causes (HIV/AIDS, malaria, syphilis, drug-susceptible tuberculosis, or multi-drug resistant tuberculosis), and to a GBD country; reported a currency year during or after 1990; and for which the comparator intervention was defined as no intervention, standard of care, or placebo. Our meta-regression analysis used all available data on 25 eligible interventions, and quantified the association between ICERs and factors at country level and intervention level. We used a five-stage statistical model that was developed to synthesise evidence on cost-effectiveness analyses, and we adapted it for smaller sample sizes by grouping interventions by cause and type (ie, prevention, diagnostics, and treatment). Using the meta-regression parameters we predicted country-specific median ICERs, IQRs, and 95% uncertainty intervals in 2019 US$ per disability-adjusted life-year (DALY) for 14 currently recommended interventions. We report ICERs in league tables with gross domestic product (GDP) per capita and country-specific thresholds.
Findings: The sample for the analysis was 1273 ratios from 144 articles, of which we included 612 ICERs from 106 articles in our meta-regression analysis. We predicted ICERs for antiretroviral therapy for prevention for two age groups and pregnant women, pre-exposure prophylaxis against HIV for two risk groups, four malaria prevention interventions, antenatal syphilis screening, two tuberculosis prevention interventions, the Xpert tuberculosis test, and chemotherapy for drug-sensitive tuberculosis. At the country level, ranking of interventions and number of interventions with a predicted median ICER below the country-specific threshold varied greatly. For instance, median ICERs for six of 14 interventions were below the country-specific threshold in Sudan, whereas 12 of 14 were below the country-specific threshold in Peru. Antenatal syphilis screening had the lowest median ICER among all 14 interventions in 81 (63%) of 128 countries, ranging from $3 (IQR 2-4) per DALY averted in Equatorial Guinea to $3473 (2244-5222) in Ukraine. Pre-exposure prophylaxis for HIV/AIDS for men who have sex with men had the highest median ICER among all interventions in 116 (91%) countries, ranging from $2326 (1077-4567) per DALY averted in Lesotho to $53 559 (23 841-108 534) in Maldives.
Interpretation: Country-specific league tables highlight the interventions that offer better value per DALY averted, and can support decision making at a country level that is more tailored to available resources than GDP per capita and country-specific thresholds. Meta-regression is a promising method to synthesise cost-effectiveness analysis results and transfer them across settings.
Funding: Bill & Melinda Gates Foundation.
Copyright © 2024 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests We declare no competing interests.
Figures






References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
