

PD-1 Inhibitor Induced Hypertrophic Lichen Planus: A Case Report
- PMID: 38877280
- PMCID: PMC11315870
- DOI: 10.1007/s40268-024-00461-x
PD-1 Inhibitor Induced Hypertrophic Lichen Planus: A Case Report
Abstract
Background and objective: PD-1 inhibitors have revolutionized cancer therapies and are being used to treat an expanding array of cancers. To best serve patients, clinicians should be familiar with the spectrum of skin manifestations associated with PD-1 inhibitor therapy. Here, we report a unique case of hypertrophic lichen planus (HLP) in a 64-year-old man treated with pembrolizumab; the presentation initially suggested a squamous cell carcinoma (SCC) morphology, then evolved into a morphology more typical of hypertrophic lichen planus. This case underscores the need for caution in diagnosing eruptive SCCs associated with PD-1 inhibitor therapy. In such instances, maintaining a high suspicion for lichenoid reactions as sequelae of PD-1 inhibitor treatment and starting an empiric trial of therapy for lichenoid dermatitis may be warranted to ensure timely management of lesions.
Methods: We describe a case of hypertrophic lichen planus mimicking squamous cell carcinoma in the setting of PD-1 inhibitory therapy with pembrolizumab. A PubMed literature review was conducted to identify other cases and determine the incidence of lichenoid reactions imitating squamous cell carcinoma in the setting of PD-1 inhibitor use.
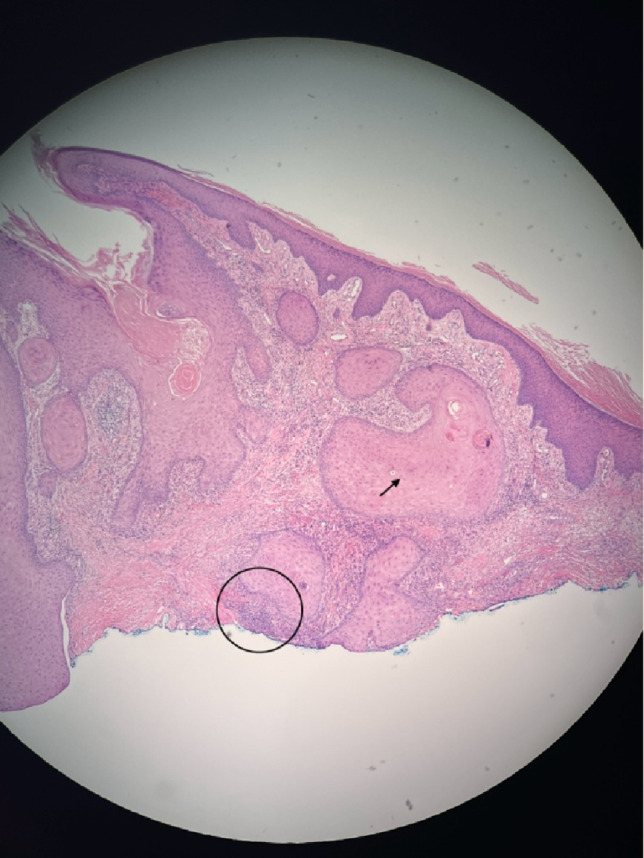
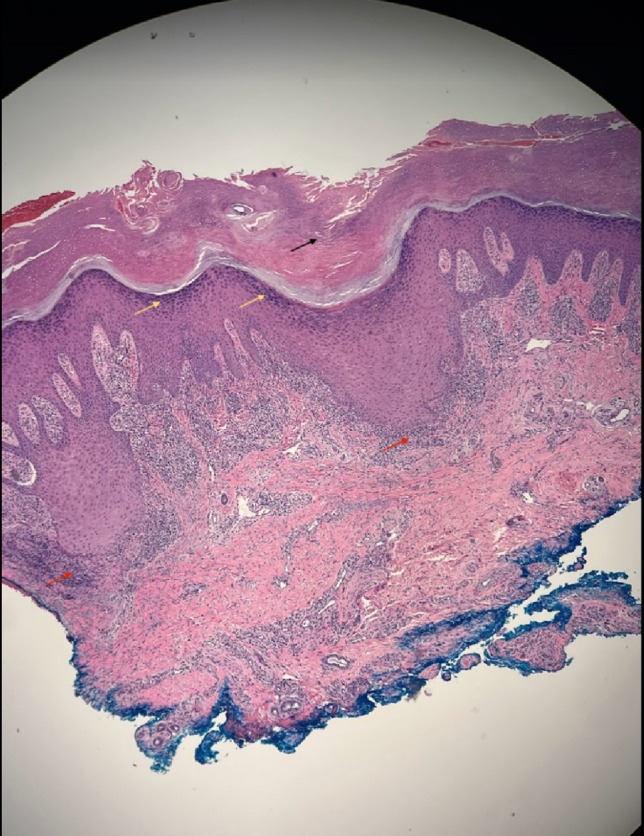
Results: Our case is one of the few available pieces of literature describing eruptive hypertrophic lichen planus imitating SCC in the setting of PD-1 inhibitor use. Initial skin nodule biopsy appeared histologically compatible with squamous cell carcinoma. Repeat biopsy of the skin lesions revealed histological features consistent with hypertrophic lichen planus. Over time, lower extremity lesions evolved into a more typical appearance of hypertrophic lichen planus. Treatment with topical 0.05% clobetasol ointment and oral acitretin 25 mg led to complete resolution of lesions within 2-3 months.
Conclusions: This case underscores the significance of maintaining vigilance for lichenoid reactions as potential sequelae of PD-1 inhibitor therapy. It highlights the variability in initial presentation and the potential for lesions to transform over time. Timely recognition and appropriate management, including high-potency topical corticosteroids and oral acitretin, are crucial for achieving favorable outcomes in patients experiencing such reactions. More studies are necessary to fully analyze the rate of HLP occurrence as a consequence of PD-1 inhibitor use.
© 2024. The Author(s).
Conflict of interest statement
Not applicable.
Figures



Similar articles
-
Hypertrophic Lichen Planus with Histological Features of Squamous Cell Carcinoma Associated with Immune Checkpoint Blockade Therapy.Oncologist. 2020 May;25(5):366-368. doi: 10.1634/theoncologist.2019-0796. Epub 2020 Feb 19. Oncologist. 2020. PMID: 32073194 Free PMC article.
-
Pembrolizumab-induced pseudoepitheliomatous eruption consistent with hypertrophic lichen planus.J Cutan Pathol. 2020 Mar;47(3):275-279. doi: 10.1111/cup.13587. Epub 2019 Oct 20. J Cutan Pathol. 2020. PMID: 31589773
-
Hypertrophic lichenoid dermatitis immune-related adverse event during combined immune checkpoint and exportin inhibitor therapy: A diagnostic pitfall for superficially invasive squamous cell carcinoma.J Cutan Pathol. 2020 Oct;47(10):954-959. doi: 10.1111/cup.13739. Epub 2020 Jun 10. J Cutan Pathol. 2020. PMID: 32394425
-
Hypertrophic Lichen Planus and Hypertrophic Skin Lesions Associated with Histological Lichenoid Infiltrate: A Case Report and Literature Review.Dermatopathology (Basel). 2025 Feb 25;12(1):8. doi: 10.3390/dermatopathology12010008. Dermatopathology (Basel). 2025. PMID: 40136318 Free PMC article. Review.
-
Squamous Cell Carcinoma Arising in Hypertrophic Lichen Planus: A Review and Analysis of 38 Cases.Dermatol Surg. 2015 Dec;41(12):1411-8. doi: 10.1097/DSS.0000000000000565. Dermatol Surg. 2015. PMID: 26551772 Review.
Cited by
-
Eruptive keratoacanthoma secondary to immune checkpoint inhibitors: a narrative review.Arch Dermatol Res. 2025 Jan 13;317(1):234. doi: 10.1007/s00403-024-03694-7. Arch Dermatol Res. 2025. PMID: 39804491 Review.
References
-
- Coleman E, Ko C, Dai F, Tomayko MM, Kluger H, Leventhal JS. Inflammatory eruptions associated with immune checkpoint inhibitor therapy: a single-institution retrospective analysis with stratification of reactions by toxicity and implications for management. J Am Acad Dermatol. 2019;80(4):990–7. 10.1016/j.jaad.2018.10.062. 10.1016/j.jaad.2018.10.062 - DOI - PMC - PubMed
-
- Shi VJ, Rodic N, Gettinger S, et al. Clinical and histologic features of lichenoid mucocutaneous eruptions due to anti-programmed cell death 1 and anti-programmed cell death ligand 1 immunotherapy. JAMA Dermatol. 2016;152(10):1128–36. 10.1001/jamadermatol.2016.2226. 10.1001/jamadermatol.2016.2226 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
