

Early safety and efficiency outcomes of a novel interdisciplinary laparoscopic resection rectopexy combined with sacrocolpopexy for women with obstructive defecation syndrome and pelvic organ prolapse: a single center study
- PMID: 38877450
- PMCID: PMC11177501
- DOI: 10.1186/s12893-024-02474-4
Early safety and efficiency outcomes of a novel interdisciplinary laparoscopic resection rectopexy combined with sacrocolpopexy for women with obstructive defecation syndrome and pelvic organ prolapse: a single center study
Abstract
Background: Obstructive defecation syndrome (ODS) defines a disturbed defecation process frequently associated with pelvic organ prolapse (POP) in women that substantially compromises quality of life. Conservative management offers limited relief and a surgical intervention may be required. This is characterized by individual approaches. AIM OF THE STUDY: This retrospective single center study evaluated the surgical and clinical short-term outcome of a novel interdisciplinary laparoscopic resection rectopexy (L-RRP) with mesh- sacrocolpopexy (L-SCP) for women suffering from ODS and POP.
Methods: The study participants underwent surgery in an interdisciplinary laparoscopic approach. Safety was the primary endpoint, assessed via postoperative morbidity classified by Clavien-Dindo scale. Secondary outcomes included evaluation of bowel function, fecal and urinary incontinence and pelvic organ prolapse status at 12 months follow-up. Additionally, a biological mesh (BM) was offered to women, who asked for an alternative to synthetic mesh material (SM).
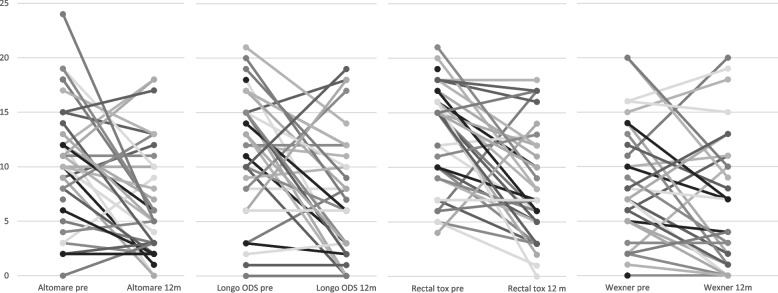
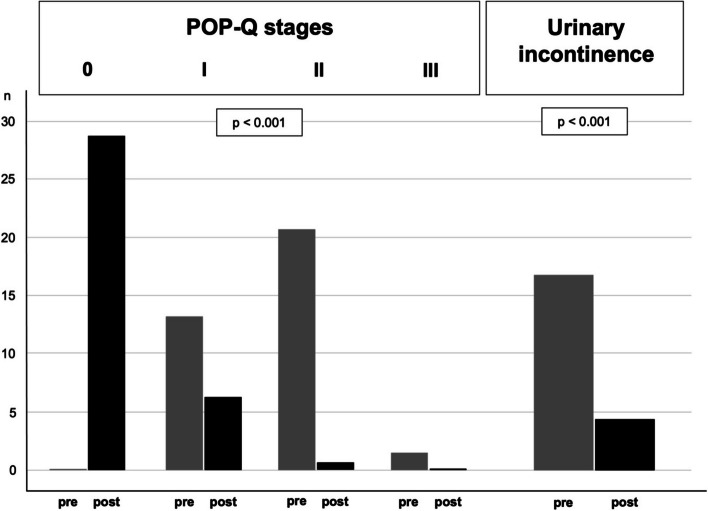
Results: Of the 44 consecutive patients requiring surgery for ODS and POP, 36 patients underwent the interdisciplinary surgical approach; 28 patients with SM and 8 patients with BM. In total 5 complications occurred, four of them were classified as minor. One minor complication was observed in the BM group. One anastomotic leakage occurred in the SM group. The two ODS scores, the bowel dysfunction score, and the incontinence score improved significantly (p = 0.006, p = 0.003, p < 0.001, and p = 0.0035, respectively). Pelvic floor anatomy was fully restored (POP-Q 0) for 29 (80%) patients after surgery. 17 patients (47%) suffered from urinary incontinence before surgery, which was restored in 13 patients (76.5%).
Conclusions: The interdisciplinary approach with L-RRP and L-SCP and the use of a BM in a small subgroup were technically feasible, safe, and effective in this single center setting. The study's retrospective design, the small sample size and the lack of comparators limit the generalizability of the findings requiring future randomized trials.
Trial registration: Retrospectively registered at clinicaltrials.gov, trial number NCT05910021, date of registration 06/10/2023.
Keywords: Biological mesh; Obstructed defecation syndrome; Pelvic organ prolapse; Resection rectopexy; Sacrocolpopexy; Synthetic mesh.
© 2024. The Author(s).
Conflict of interest statement
Sebastian Ludwig received honoraria for speaking at symposia from the FEG Textiltechnik GmbH Aachen, Germany. All other authors declare that they have no competing interests.
Figures



Similar articles
-
Laparoscopic resection rectopexy (RRP) combined with mesh sacrocolpopexy (SCP) for obstructed defecation syndrome with pelvic organ prolapse in an interdisciplinary approach.Facts Views Vis Obgyn. 2024 Jun;16(2):231-236. doi: 10.52054/FVVO.16.2.017. Facts Views Vis Obgyn. 2024. PMID: 38950538 Free PMC article.
-
Laparoscopic sacrocolpopexy plus ventral rectopexy as combined treatment for multicompartment pelvic organ prolapse.Tech Coloproctol. 2020 Jun;24(6):573-584. doi: 10.1007/s10151-020-02199-5. Epub 2020 Apr 13. Tech Coloproctol. 2020. PMID: 32285229
-
Bowel function after laparoscopic posterior sutured rectopexy versus ventral mesh rectopexy for rectal prolapse: a double-blind, randomised single-centre study.Lancet Gastroenterol Hepatol. 2016 Dec;1(4):291-297. doi: 10.1016/S2468-1253(16)30085-1. Epub 2016 Oct 4. Lancet Gastroenterol Hepatol. 2016. PMID: 28404199 Clinical Trial.
-
Diagnosis and management of complications following pelvic organ prolapse surgery using a synthetic mesh: French national guidelines for clinical practice.Eur J Obstet Gynecol Reprod Biol. 2024 Mar;294:170-179. doi: 10.1016/j.ejogrb.2024.01.015. Epub 2024 Jan 17. Eur J Obstet Gynecol Reprod Biol. 2024. PMID: 38280271 Review.
-
Sexual function after pelvic organ prolapse surgery: a systematic review comparing different approaches to pelvic floor repair.Am J Obstet Gynecol. 2021 Nov;225(5):475.e1-475.e19. doi: 10.1016/j.ajog.2021.05.042. Epub 2021 Jun 2. Am J Obstet Gynecol. 2021. PMID: 34087227
Cited by
-
Improvement in functional and mental outcomes after resection rectopexy for obstructive defecation syndrome ODS.Sci Rep. 2025 Aug 18;15(1):30184. doi: 10.1038/s41598-025-15037-1. Sci Rep. 2025. PMID: 40825813 Free PMC article.
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
