

Unlocking the potential of robotic-assisted bronchoscopy: overcoming challenging anatomy and locations
- PMID: 38877690
- PMCID: PMC11179493
- DOI: 10.1177/17534666241259369
Unlocking the potential of robotic-assisted bronchoscopy: overcoming challenging anatomy and locations
Abstract
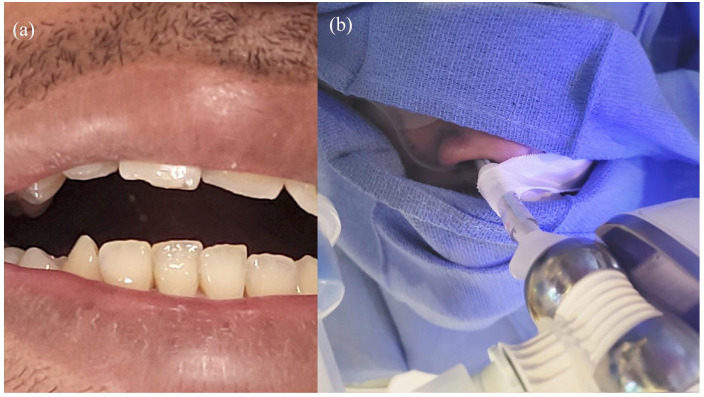
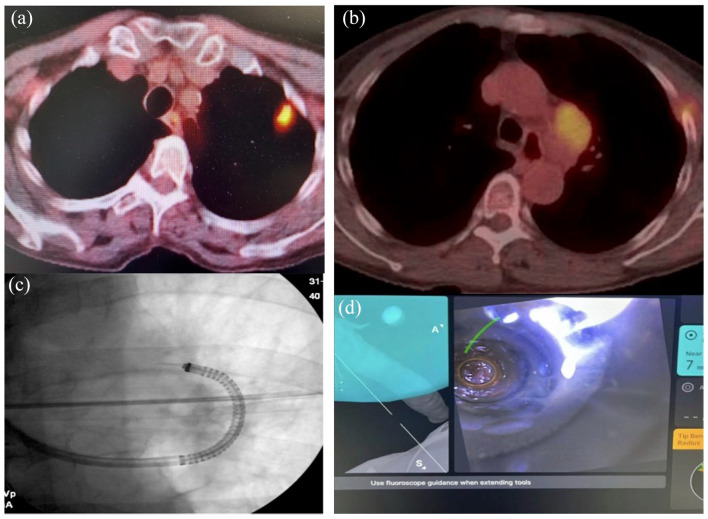
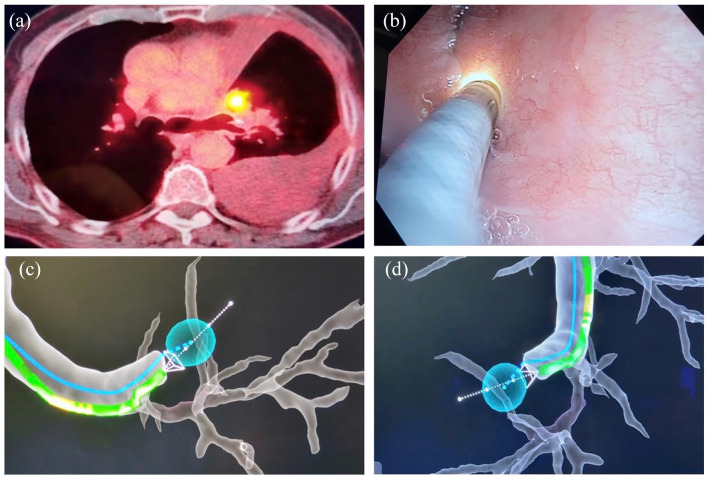
Robotic-assisted bronchoscopy (RAB) was recently added to the armamentarium of tools used in sampling peripheral lung nodules. Protocols and guidelines have since been published advocating use of large oral artificial airways, use of confirmatory technologies such as radial endobronchial ultrasound (R-EBUS), and preferably limiting sampling to pulmonary parenchymal lesions. We present three clinical cases where RAB was used unconventionally to sample pulmonary nodules in unusual locations and in patients with challenging airway anatomy. In case 1, we introduced the ion catheter through a nasal airway in a patient with trismus. In case 2, we established a diagnosis by sampling a station 5 lymph node, and in case 3, we sampled a lesion located behind an airway stump from previous thoracic surgery. All three patients would have presented significant challenges for alternative biopsy modalities such as CT-guided needle biopsy or video-assisted thoracic surgery.
Keywords: biopsy; bronchoscopy; robotic bronchoscopy.
Conflict of interest statement
The author declares that there is no conflict of interest.
Figures
Similar articles
-
Procedural times with robotic-assisted bronchoscopy: a high volume single-center study.Ther Adv Respir Dis. 2024 Jan-Dec;18:17534666241277668. doi: 10.1177/17534666241277668. Ther Adv Respir Dis. 2024. PMID: 39235434 Free PMC article.
-
Robotic Bronchoscopy for Peripheral Pulmonary Lesions: A Multicenter Pilot and Feasibility Study (BENEFIT).Chest. 2021 Feb;159(2):845-852. doi: 10.1016/j.chest.2020.08.2047. Epub 2020 Aug 19. Chest. 2021. PMID: 32822675 Free PMC article.
-
Robotic bronchoscopy: Evolution of advanced diagnostic technologies for pulmonary lesions.Best Pract Res Clin Anaesthesiol. 2024 Mar;38(1):38-46. doi: 10.1016/j.bpa.2024.05.002. Epub 2024 May 10. Best Pract Res Clin Anaesthesiol. 2024. PMID: 39764823 Review.
-
First Human Use of a New Robotic-Assisted Fiber Optic Sensing Navigation System for Small Peripheral Pulmonary Nodules.Respiration. 2019;98(2):142-150. doi: 10.1159/000498951. Epub 2019 Jul 26. Respiration. 2019. PMID: 31352444
-
Tissue diagnosis of suspected lung cancer: selecting between bronchoscopy, transthoracic needle aspiration, and resectional biopsy.Respir Care Clin N Am. 2003 Mar;9(1):51-76. doi: 10.1016/s1078-5337(02)00083-7. Respir Care Clin N Am. 2003. PMID: 12820712 Review.
Cited by
-
Staging Aortopulmonary Lymph Nodes With Robotic-Assisted Bronchoscopy: A Case Report and Literature Review.Respirol Case Rep. 2025 Feb 7;13(2):e70109. doi: 10.1002/rcr2.70109. eCollection 2025 Feb. Respirol Case Rep. 2025. PMID: 39926300 Free PMC article.
References
-
- Ali MS, Ghori UK, Wayne MT, et al.. Diagnostic performance and safety profile of robotic-assisted bronchoscopy: a systematic review and meta-analysis. Ann Am Thorac Soc 2023; 20: 1801–1812. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
