

Derivation and Internal Validation of a Novel Risk Assessment Tool to Identify Infants and Young Children at Risk for Post-Discharge Mortality in Dar es Salaam, Tanzania and Monrovia, Liberia
- PMID: 38878962
- PMCID: PMC11415288
- DOI: 10.1016/j.jpeds.2024.114147
Derivation and Internal Validation of a Novel Risk Assessment Tool to Identify Infants and Young Children at Risk for Post-Discharge Mortality in Dar es Salaam, Tanzania and Monrovia, Liberia
Abstract
Objective: To derive and validate internally a novel risk assessment tool to identify young children at risk for all-cause mortality ≤60 days of discharge from hospitals in sub-Saharan Africa.
Study design: We performed a prospective observational cohort study of children aged 1-59 months discharged from Muhimbili National Hospital in Dar es Salaam, Tanzania and John F. Kennedy Medical Center in Monrovia, Liberia (2019-2022). Caregivers received telephone calls up to 60 days after discharge to ascertain participant vital status. We collected socioeconomic, demographic, clinical, and anthropometric data during hospitalization. Candidate variables with P < .20 in bivariate analyses were included in a multivariable logistic regression model with best subset selection to identify risk factors for the outcome. We internally validated our tool using bootstrapping with 500 repetitions.
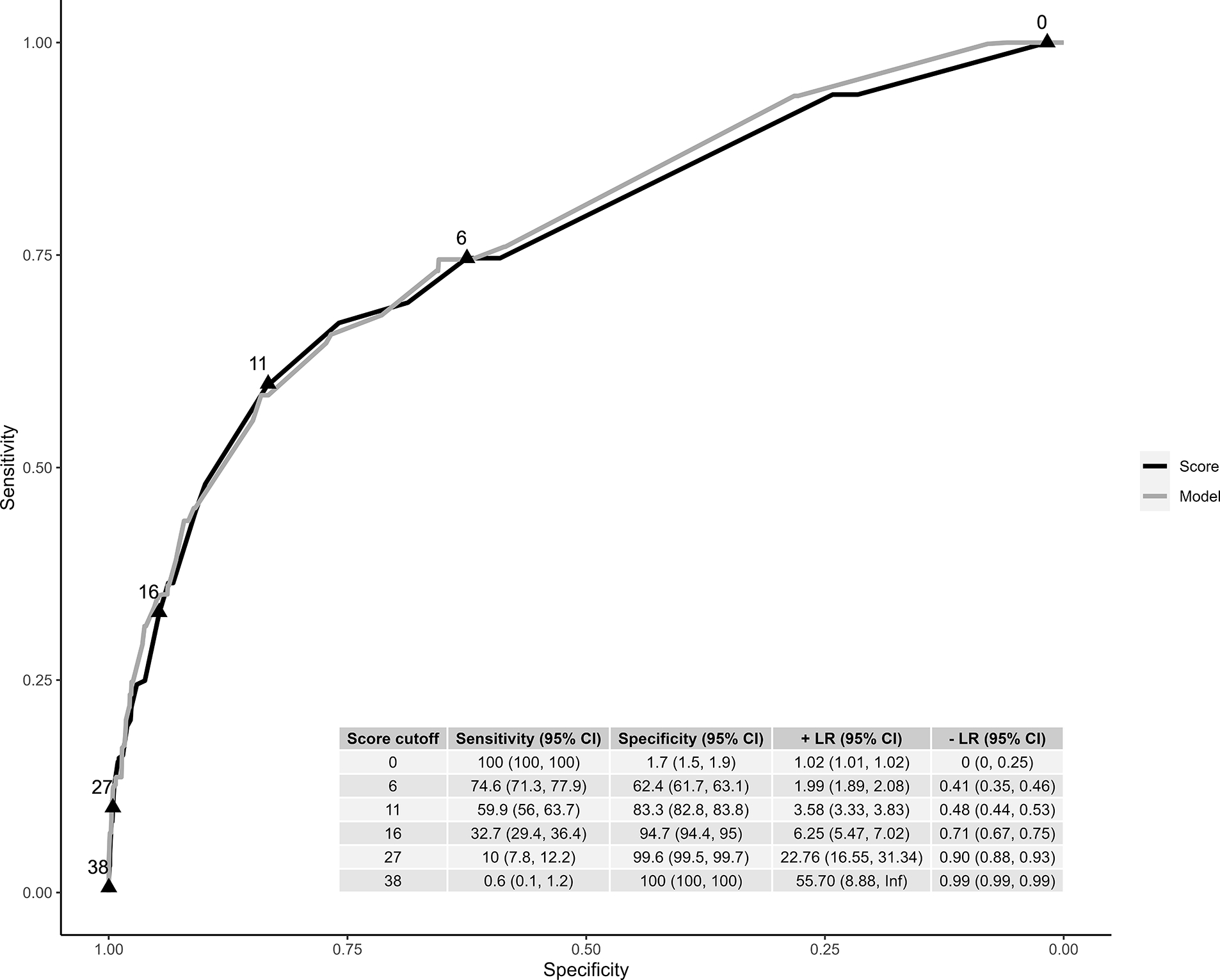
Results: There were 1933 young children enrolled in the study. The median (IQR) age was 11 (4, 23) months and 58.7% were males. In total, 67 (3.5%) died during follow-up. Ten variables contributed to our tool (total possible score 82). Cancer (aOR 10.6, 95% CI 2.58, 34.6), pedal edema (aOR 6.94, 95% CI 1.69, 22.6), and leaving against medical advice (aOR 6.46, 95% CI 2.46, 15.3) were most predictive of post-discharge mortality. Our risk assessment tool demonstrated good discriminatory value (optimism corrected area under the receiver operating characteristic curve 0.77), high precision, and sufficient calibration.
Conclusions: After validation, this tool may be used to identify young children at risk for post-discharge mortality to direct resources for follow-up of high-risk children.
Keywords: Liberia; Tanzania; child; infant; mortality; post-discharge; risk assessment tools.
Copyright © 2024 Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest C.P.D is a member of the Editorial Board of the Journal of Pediatrics but played no role in the handling of this manuscript. The other authors declare no conflicts of interest. This study was funded by the National Institutes of Health (K24 DK104676 and P30 DK040561 to CPD, K24 AT009893 to CRM, and K23HL173694 to CAR), the Boston Children's Hospital Global Health Program to CAR, the Palfrey Fund for Child Health Advocacy to CAR, and the Emory Pediatric Research Alliance Junior Faculty Focused Award to CAR. This work was presented, in part, as a platform presentation at the American Academy of Pediatrics National Conference & Exhibition in October 2023 in Washington DC.
Figures


References
-
- Wiens MO, Kissoon N, Kabakyenga J. Smart Hospital Discharges to Address a Neglected Epidemic in Sepsis in Low- and Middle-Income Countries. JAMA Pediatr 2018;172:213–214. - PubMed
-
- Maguire JL, Kulik DM, Laupacis A, Kuppermann N, Uleryk EM, Parkin PC. Clinical prediction rules for children: A systematic review. Pediatrics 2011;128:e666–e677. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
