

A Systematic Review and Bayesian Network Meta-Analysis Comparing In-Person, Remote, and Blended Interventions in Physical Activity, Diet, Education, and Behavioral Modification on Gestational Weight Gain among Overweight or Obese Pregnant Individuals
- PMID: 38879168
- PMCID: PMC11267029
- DOI: 10.1016/j.advnut.2024.100253
A Systematic Review and Bayesian Network Meta-Analysis Comparing In-Person, Remote, and Blended Interventions in Physical Activity, Diet, Education, and Behavioral Modification on Gestational Weight Gain among Overweight or Obese Pregnant Individuals
Abstract
Background: Despite the well-documented adverse outcomes associated with obesity during pregnancy, this condition remains a promising modifiable risk factor.
Objectives: The aim of this study was to ascertain the most effective treatment modalities for gestational weight gain (GWG) in pregnant women classified as overweight or obese.
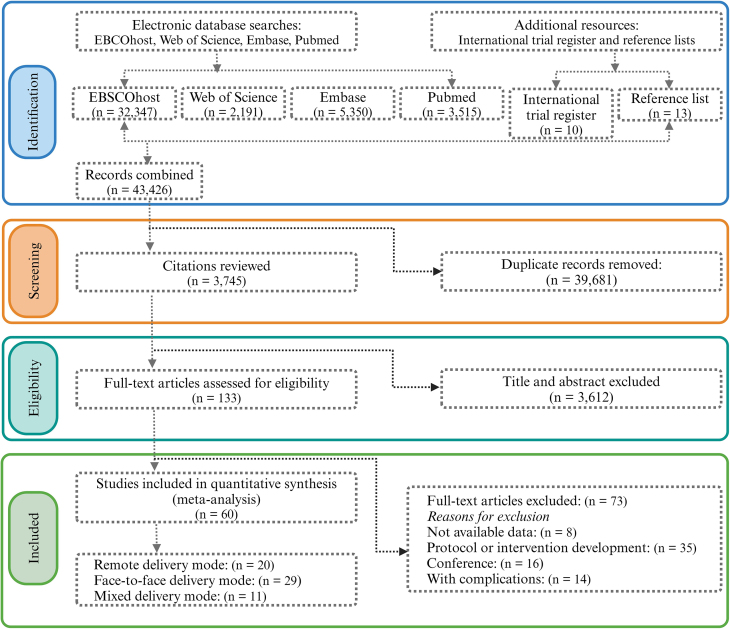
Methods: A systematic search was conducted across 4 electronic databases: Embase, EBSCOhost, PubMed, and Web of Science. To assess the quality of evidence, the Confidence In Network Meta-Analysis (CINeMA) approach, grounded in the Grading of Recommendations Assessment, Development, and Evaluation framework, was employed. A Bayesian network meta-analysis was conducted to synthesize the comparative effectiveness of treatment modalities based on GWG outcomes.
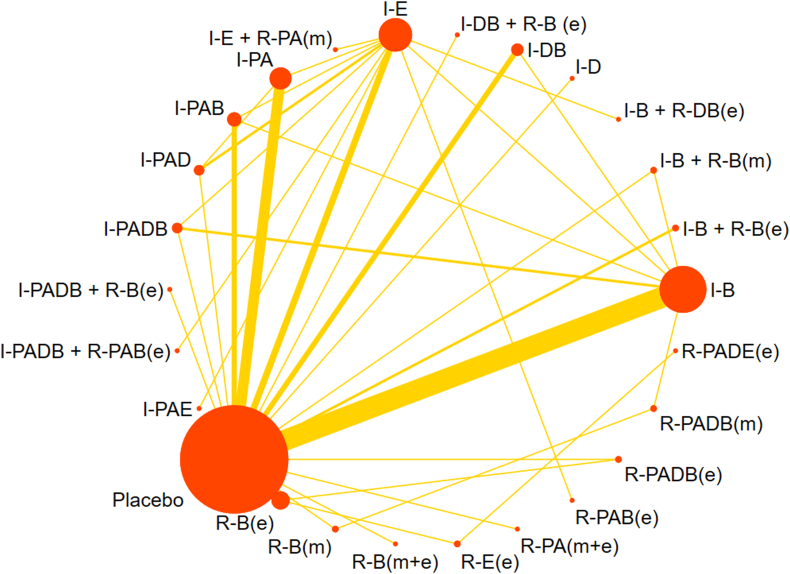
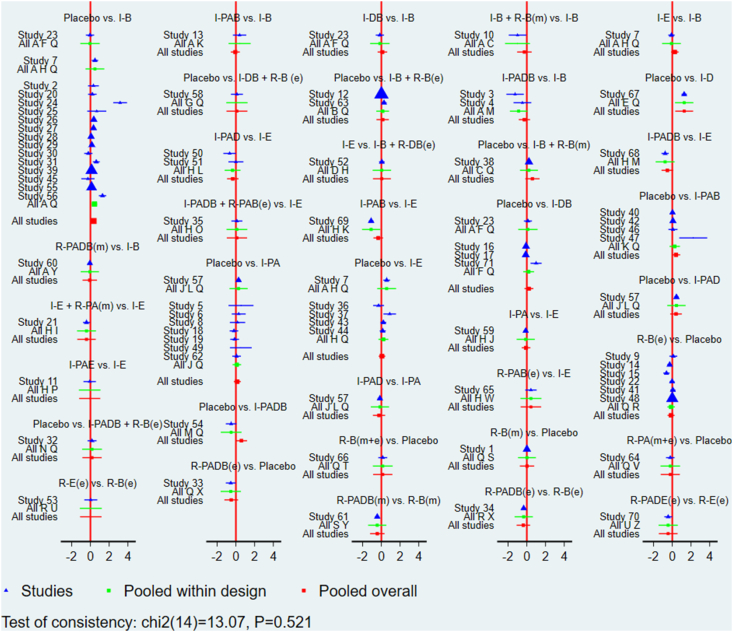
Results: The analysis incorporated 60 randomized controlled trials, encompassing 16,615 participants. Modes of intervention administration were classified as remote (R: eHealth [e] and mHealth [m]), in-person (I), and a combination of both (I+R). The interventions comprised 5 categories: education (E), physical activity (PA), dietary (D), behavior modification (B), and combinations thereof. The quality of the evidence, as evaluated by CINeMA, ranged from very low to high. Compared to the control group, the I-D intervention (mean difference [MD]: -1.27; 95% confidence interval [CI]: -2.23, -0.32), I-PADB (MD: -0.60, 95% CI: -1.19, -0.00), and I-B (MD: -0.34, 95% CI: -0.57, -0.10) interventions showed significant efficacy in reducing GWG.
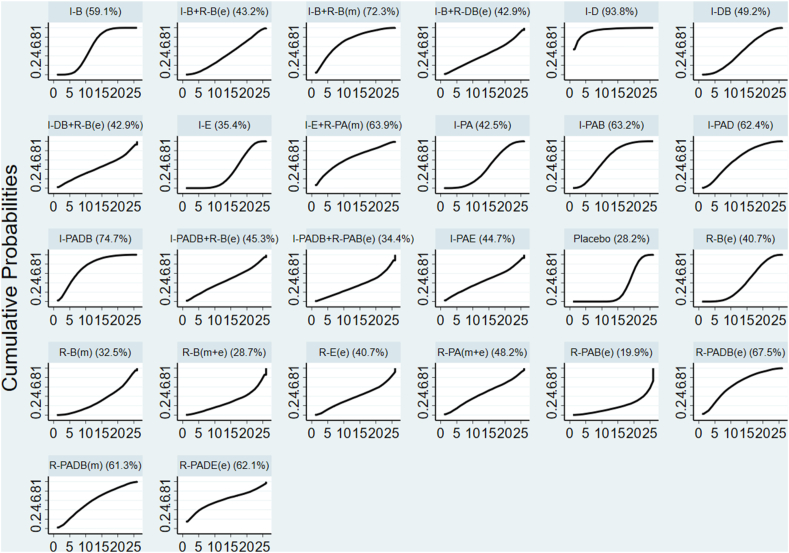
Conclusions: Preliminary findings suggest that the I-D intervention is the most efficacious in managing GWG among pregnant women who are overweight or obese, followed by I-PADB and I-B+R-B(m) treatments. These conclusions are drawn from evidence of limited quality and directness, including insufficient data on PA components used in the interventions. Owing to the absence of robust, direct evidence delineating significant differences among various GWG management strategies, it is tentatively proposed that the I-D intervention is likely the most effective approach. This study was registered with PROSPERO as CRD42023473627.
Keywords: diet; gestational weight gain; lifestyle; physical activity; pregnancy.
Copyright © 2024 The Author(s). Published by Elsevier Inc. All rights reserved.
Figures
Similar articles
-
The effectiveness of behavioral modification interventions for managing weight gain in pregnant women with overweight or obesity: a systematic review and Bayesian network meta-analysis.Health Psychol Rev. 2025 Jun;19(2):448-462. doi: 10.1080/17437199.2025.2474023. Epub 2025 Mar 5. Health Psychol Rev. 2025. PMID: 40042860
-
Drugs for preventing postoperative nausea and vomiting in adults after general anaesthesia: a network meta-analysis.Cochrane Database Syst Rev. 2020 Oct 19;10(10):CD012859. doi: 10.1002/14651858.CD012859.pub2. Cochrane Database Syst Rev. 2020. PMID: 33075160 Free PMC article.
-
Lifestyle interventions for the treatment of women with gestational diabetes.Cochrane Database Syst Rev. 2017 May 4;5(5):CD011970. doi: 10.1002/14651858.CD011970.pub2. Cochrane Database Syst Rev. 2017. PMID: 28472859 Free PMC article.
-
Combined diet and exercise interventions for preventing gestational diabetes mellitus.Cochrane Database Syst Rev. 2017 Nov 13;11(11):CD010443. doi: 10.1002/14651858.CD010443.pub3. Cochrane Database Syst Rev. 2017. PMID: 29129039 Free PMC article.
-
Metformin for women who are overweight or obese during pregnancy for improving maternal and infant outcomes.Cochrane Database Syst Rev. 2018 Jul 24;7(7):CD010564. doi: 10.1002/14651858.CD010564.pub2. Cochrane Database Syst Rev. 2018. PMID: 30039871 Free PMC article.
Cited by
-
Association of obesity with ropivacaine and sufentanil EC50 in labor analgesia: a single-center prospective study.Eur J Clin Pharmacol. 2025 Mar;81(3):419-428. doi: 10.1007/s00228-024-03800-8. Epub 2025 Jan 8. Eur J Clin Pharmacol. 2025. PMID: 39774874
-
Advances in Epidural Labor Analgesia for Obese Parturients.J Pain Res. 2024 Dec 7;17:4141-4147. doi: 10.2147/JPR.S495666. eCollection 2024. J Pain Res. 2024. PMID: 39664370 Free PMC article. Review.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
