

Genetics and Pathophysiological Mechanisms of Lipoprotein(a)-Associated Cardiovascular Risk
- PMID: 38879448
- PMCID: PMC11255763
- DOI: 10.1161/JAHA.123.033654
Genetics and Pathophysiological Mechanisms of Lipoprotein(a)-Associated Cardiovascular Risk
Abstract
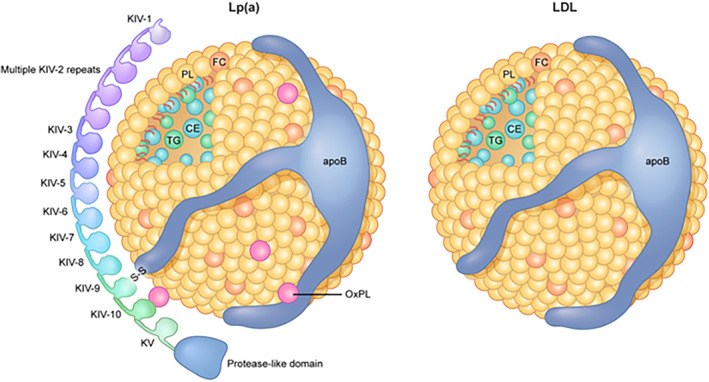
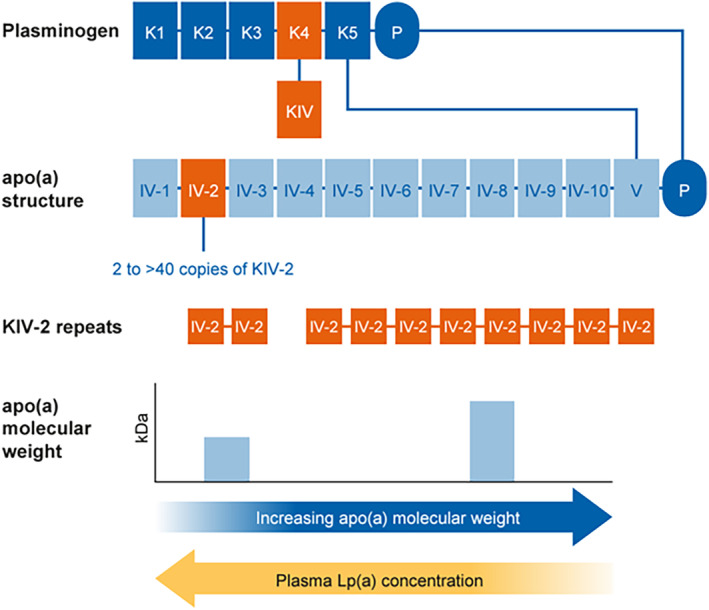
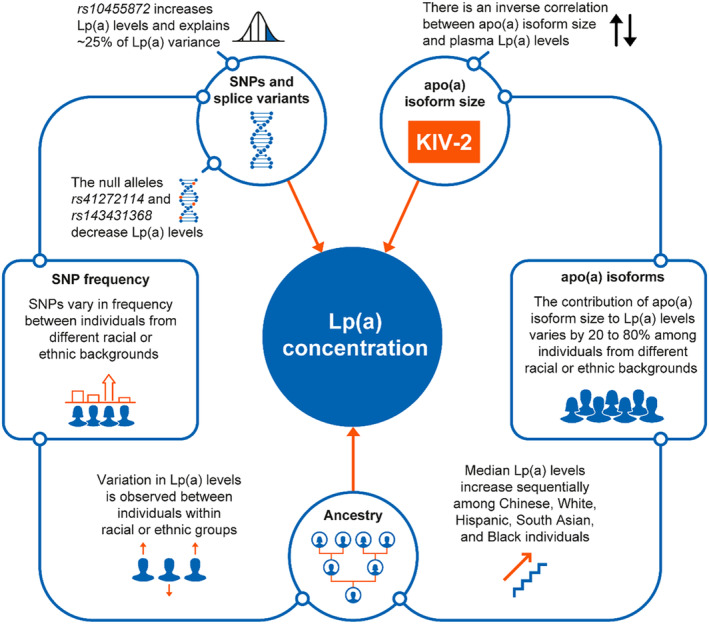
Elevated lipoprotein(a) is a genetically transmitted codominant trait that is an independent risk driver for cardiovascular disease. Lipoprotein(a) concentration is heavily influenced by genetic factors, including LPA kringle IV-2 domain size, single-nucleotide polymorphisms, and interleukin-1 genotypes. Apolipoprotein(a) is encoded by the LPA gene and contains 10 subtypes with a variable number of copies of kringle -2, resulting in >40 different apolipoprotein(a) isoform sizes. Genetic loci beyond LPA, such as APOE and APOH, have been shown to impact lipoprotein(a) levels. Lipoprotein(a) concentrations are generally 5% to 10% higher in women than men, and there is up to a 3-fold difference in median lipoprotein(a) concentrations between racial and ethnic populations. Nongenetic factors, including menopause, diet, and renal function, may also impact lipoprotein(a) concentration. Lipoprotein(a) levels are also influenced by inflammation since the LPA promoter contains an interleukin-6 response element; interleukin-6 released during the inflammatory response results in transient increases in plasma lipoprotein(a) levels. Screening can identify elevated lipoprotein(a) levels and facilitate intensive risk factor management. Several investigational, RNA-targeted agents have shown promising lipoprotein(a)-lowering effects in clinical studies, and large-scale lipoprotein(a) testing will be fundamental to identifying eligible patients should these agents become available. Lipoprotein(a) testing requires routine, nonfasting blood draws, making it convenient for patients. Herein, we discuss the genetic determinants of lipoprotein(a) levels, explore the pathophysiological mechanisms underlying the association between lipoprotein(a) and cardiovascular disease, and provide practical guidance for lipoprotein(a) testing.
Keywords: atherosclerotic cardiovascular disease; cardiovascular risk; coronary heart disease; genetics; lipoprotein(a); oxidized phospholipids; single nucleotide polymorphisms.
Figures
References
-
- Catapano AL, Daccord M, Damato E, Humphries SE, Neely RDG, Nordestgaard BG, Pistollato M, Steinhagen‐Thiessen E. How should public health recommendations address Lp(a) measurement, a causative risk factor for cardiovascular disease (CVD)? Atherosclerosis. 2022;349:136–143. doi: 10.1016/j.atherosclerosis.2022.02.013 - DOI - PubMed
-
- Tsao CW, Aday AW, Almarzooq ZI, Anderson CAM, Arora P, Avery CL, Baker‐Smith CM, Beaton AZ, Boehme AK, Buxton AE, et al. Heart disease and stroke Statistics‐2023 update: a report from the American Heart Association. Circulation. 2023;147:e93–e621. doi: 10.1161/cir.0000000000001123 - DOI - PMC - PubMed
-
- Tsimikas S, Fazio S, Ferdinand KC, Ginsberg HN, Koschinsky ML, Marcovina SM, Moriarty PM, Rader DJ, Remaley AT, Reyes‐Soffer G, et al. NHLBI working group recommendations to reduce lipoprotein(a)‐mediated risk of cardiovascular disease and aortic stenosis. J Am Coll Cardiol. 2018;71:177–192. doi: 10.1016/j.jacc.2017.11.014 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
