

Role of Antitroponin Antibodies and Macrotroponin in the Clinical Interpretation of Cardiac Troponin
- PMID: 38879450
- PMCID: PMC11255741
- DOI: 10.1161/JAHA.123.035128
Role of Antitroponin Antibodies and Macrotroponin in the Clinical Interpretation of Cardiac Troponin
Abstract
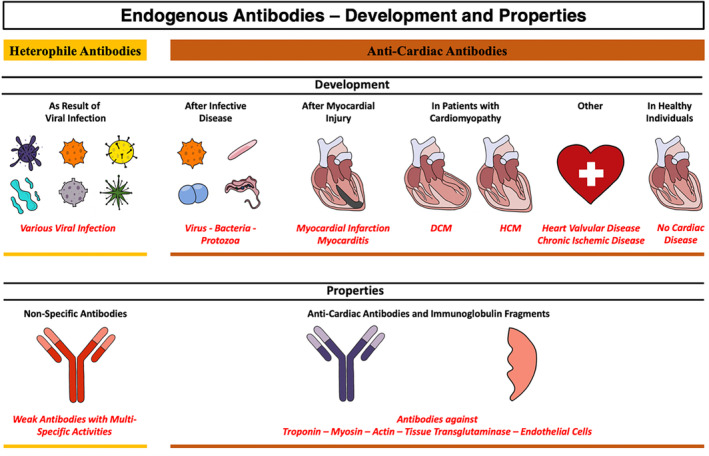
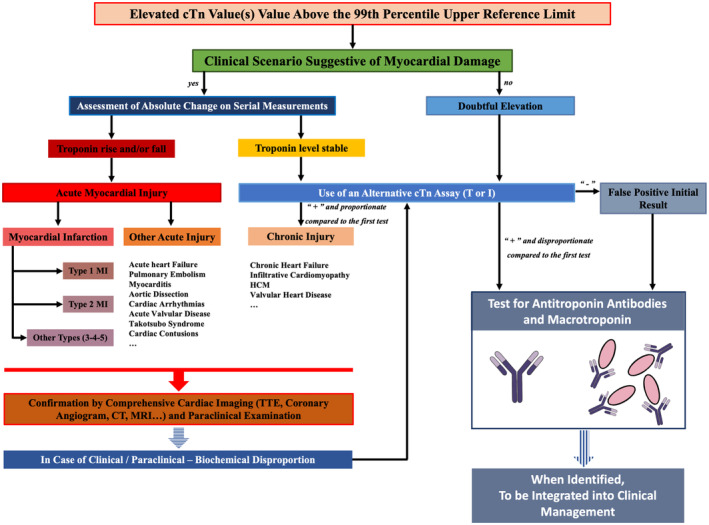
Cardiac troponin is extensively used as a biomarker in modern medicine due to its diagnostic capability for myocardial injury, as well as its predictive and prognostic value for cardiac diseases. However, heterophile antibodies, antitroponin antibodies, and macrotroponin complexes can be observed both in seemingly healthy individuals and patients with cardiac diseases, potentially leading to false positive or disproportionate elevation of cTn (cardiac troponin) assay results and introducing discrepancies in clinical interpretations with impact on medical management. In this review article, we describe the possible mechanisms of cTn release and the sources of variations in the assessment of circulating cTn levels. We also explore the pathophysiological mechanisms underlying antitroponin antibody development and discuss the influence exerted by macrotroponin complexes on the results of immunoassays. Additionally, we explore approaches to detect these complexes by presenting various clinical scenarios encountered in routine clinical practice. Finally, unsolved questions about the development, prevalence, and clinical significance of cardiac autoantibodies are discussed.
Keywords: antitroponin antibodies; biomarker; cardiac troponin; macrotroponin; myocardial infarction; myocardial injury; myocarditis.
Figures




Similar articles
-
Effect of macrotroponin on the utility of cardiac troponin I as a prognostic biomarker for long term total and cardiovascular disease mortality.Pathology. 2021 Dec;53(7):860-866. doi: 10.1016/j.pathol.2021.04.005. Epub 2021 Jul 14. Pathology. 2021. PMID: 34272050
-
Change in troponin concentrations in patients with macrotroponin: An in vitro mixing study.Clin Biochem. 2020 Nov;85:43-48. doi: 10.1016/j.clinbiochem.2020.08.012. Epub 2020 Aug 27. Clin Biochem. 2020. PMID: 32861681
-
Macrotroponin causing elevation in cardiac troponin I.Can J Cardiol. 2014 Aug;30(8):956.e5-6. doi: 10.1016/j.cjca.2014.03.037. Epub 2014 Apr 2. Can J Cardiol. 2014. PMID: 24999169
-
High-sensitivity cardiac troponin assays: From improved analytical performance to enhanced risk stratification.Crit Rev Clin Lab Sci. 2017 May;54(3):143-172. doi: 10.1080/10408363.2017.1285268. Epub 2017 May 1. Crit Rev Clin Lab Sci. 2017. PMID: 28457177 Review.
-
Cardiac troponin level elevations not related to acute coronary syndromes.Nat Rev Cardiol. 2013 Nov;10(11):623-34. doi: 10.1038/nrcardio.2013.129. Epub 2013 Aug 27. Nat Rev Cardiol. 2013. PMID: 23979214 Review.
Cited by
-
Interfering heterophile antibodies as the cause of persistently falsely elevated high-sensitivity troponin I on Alinity i: a case report.Biochem Med (Zagreb). 2025 Jun 15;35(2):021001. doi: 10.11613/BM.2025.021001. Biochem Med (Zagreb). 2025. PMID: 40520654 Free PMC article.
-
Cardiac involvement in female elite athletes with carrier status of Duchenne muscular dystrophy.Front Cardiovasc Med. 2025 Jul 7;12:1606994. doi: 10.3389/fcvm.2025.1606994. eCollection 2025. Front Cardiovasc Med. 2025. PMID: 40693222 Free PMC article. Review.
-
Cardiac Troponin Levels in Patients with Chronic Kidney Disease: "Markers of High Risk or Just Noise''?Diagnostics (Basel). 2024 Oct 18;14(20):2316. doi: 10.3390/diagnostics14202316. Diagnostics (Basel). 2024. PMID: 39451639 Free PMC article. Review.
-
False Troponin Elevation in Pediatric Patients: A Long-Term Biochemical Conundrum Without Cardiac Effects.Diagnostics (Basel). 2025 Jul 22;15(15):1847. doi: 10.3390/diagnostics15151847. Diagnostics (Basel). 2025. PMID: 40804811 Free PMC article.
-
High sensitivity troponins and mortality in the population with metabolic dysfunction-associated steatotic liver disease.Sci Rep. 2024 Aug 22;14(1):19541. doi: 10.1038/s41598-024-70645-7. Sci Rep. 2024. PMID: 39174636 Free PMC article.
References
-
- Thygesen K, Alpert JS, Jaffe AS, Chaitman BR, Bax JJ, Morrow DA, White HD. Executive group on behalf of the joint European Society of Cardiology/American College of Cardiology/American Heart Association/world heart federation task force for the universal definition of myocardial I. Fourth universal definition of myocardial infarction (2018). J Am Coll Cardiol. 2018;72:2231–2264. doi: 10.1016/j.jacc.2018.08.1038 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
