

Comparison of Endovascular Therapy and Open Surgical Revascularization in Patients With Acute Superior Mesenteric Artery Occlusion: A Large-Scale Analysis Based on the JROAD-DPC Database
- PMID: 38879458
- PMCID: PMC11255773
- DOI: 10.1161/JAHA.124.035017
Comparison of Endovascular Therapy and Open Surgical Revascularization in Patients With Acute Superior Mesenteric Artery Occlusion: A Large-Scale Analysis Based on the JROAD-DPC Database
Abstract
Background: Acute mesenteric ischemia is rare, and few large-scale trials have evaluated endovascular therapy (EVT) and open surgical revascularization (OS). This study aimed to assess clinical outcomes after EVT or OS for acute superior mesenteric artery occlusion and identify predictors of mortality and bowel resection.
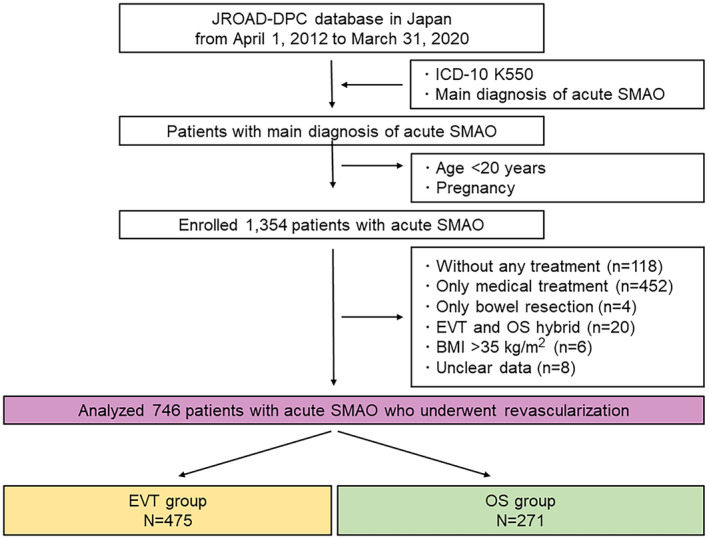
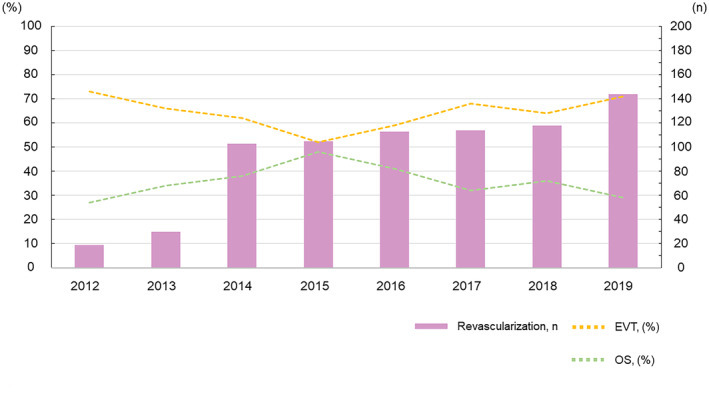
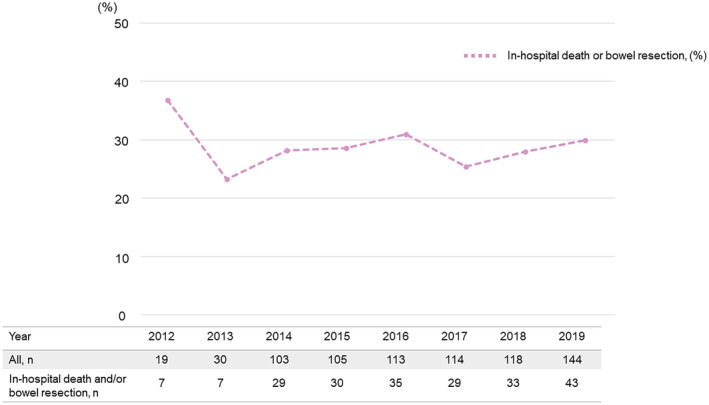
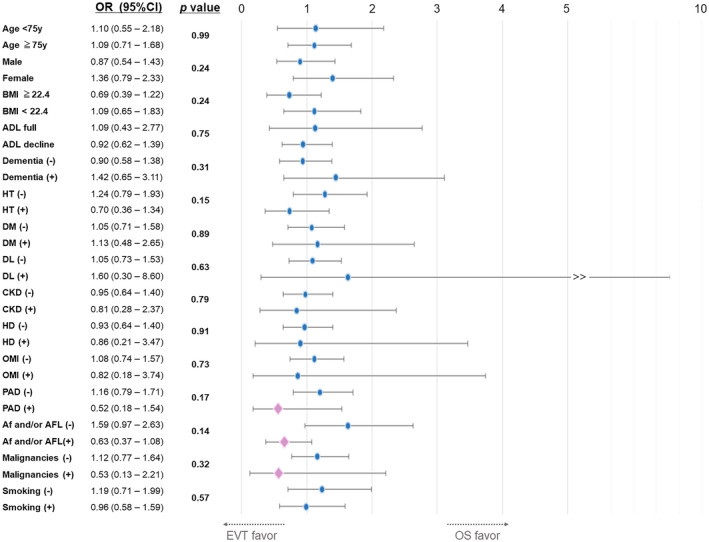
Methods and results: Data from the Japanese Registry of All Cardiac and Vascular Diseases-Diagnosis Procedure Combination (JROAD-DPC) database from April 2012 to March 2020 were retrospectively analyzed. Overall, 746 patients with acute superior mesenteric artery occlusion who underwent revascularization were classified into 2 groups: EVT (n=475) or OS (n=271). The primary clinical outcome was in-hospital mortality. The secondary outcomes were bowel resection, bleeding complications (transfusion or endoscopic hemostasis), major adverse cardiovascular events, hospitalization duration, and cost. The in-hospital death or bowel resection rate was ≈30%. In-hospital mortality (22.5% versus 21.4%, P=0.72), bowel resection (8.2% versus 8.5%, P=0.90), and major adverse cardiovascular events (11.6% versus 9.2%, P=0.32) were comparable between the EVT and OS groups. Hospitalization duration in the EVT group was 6 days shorter than that in the OS group, and total hospitalization cost was 0.88 million yen lower. Interaction analyses revealed that EVT and OS had no significant difference in terms of in-hospital death in patients with thromboembolic and atherothrombotic characteristics. Advanced age, decreased activities of daily living, chronic kidney disease, and old myocardial infarction were significant predictive factors for in-hospital mortality. Diabetes was a predictor of bowel resection after revascularization.
Conclusions: EVT was comparable to OS in terms of clinical outcomes in patients with acute superior mesenteric artery occlusion. Some predictive factors for mortality or bowel resection were obtained.
Registration: URL: www.umin.ac.jp/ctr/; Unique Identifier: UMIN000045240.
Keywords: acute superior mesenteric artery occlusion; bowel resection; endovascular therapy; in‐hospital mortality; open surgical revascularization.
Figures
Similar articles
-
Endovascular Revascularization with Stent Implantation in Patients with Acute Mesenteric Ischemia due to Acute Arterial Thrombosis: Clinical Outcome and Predictive Factors.Cardiovasc Intervent Radiol. 2021 Jul;44(7):1030-1038. doi: 10.1007/s00270-021-02824-2. Epub 2021 Apr 6. Cardiovasc Intervent Radiol. 2021. PMID: 33825061 Free PMC article.
-
Editor's Choice - Comparison of Clinical Outcomes in Patients with Acute Lower Limb Ischaemia Undergoing Endovascular Therapy and Open Surgical Revascularisation: A Large Scale Analysis in Japan.Eur J Vasc Endovasc Surg. 2024 Dec;68(6):748-756. doi: 10.1016/j.ejvs.2024.08.039. Epub 2024 Aug 30. Eur J Vasc Endovasc Surg. 2024. PMID: 39218296
-
Results of retrograde open mesenteric stenting for acute thrombotic mesenteric ischemia.J Vasc Surg. 2019 Apr;69(4):1137-1142. doi: 10.1016/j.jvs.2018.07.058. Epub 2019 Feb 15. J Vasc Surg. 2019. PMID: 30777691
-
Surgical management of peritonitis secondary to acute superior mesenteric artery occlusion.World J Gastroenterol. 2014 Aug 7;20(29):9936-41. doi: 10.3748/wjg.v20.i29.9936. World J Gastroenterol. 2014. PMID: 25110423 Free PMC article. Review.
-
Contemporary Management of Acute Mesenteric Ischemia in the Endovascular Era.Vasc Endovascular Surg. 2019 Jan;53(1):42-50. doi: 10.1177/1538574418805228. Epub 2018 Oct 25. Vasc Endovascular Surg. 2019. PMID: 30360689 Review.
Cited by
-
Outcomes after open and endovascular treatment for mesenteric artery embolism patients: a retrospective inverse probability of treatment-weighted analysis.Eur J Trauma Emerg Surg. 2024 Dec;50(6):2883-2893. doi: 10.1007/s00068-024-02647-z. Epub 2024 Aug 27. Eur J Trauma Emerg Surg. 2024. PMID: 39190060
-
Comparison between endovascular and surgical treatment of acute arterial occlusive mesenteric ischemia.World J Emerg Surg. 2025 Jun 2;20(1):46. doi: 10.1186/s13017-025-00616-4. World J Emerg Surg. 2025. PMID: 40452055 Free PMC article.
-
Tricky acute mesenteric ischemia: what can we do?Gastroenterol Rep (Oxf). 2025 Jul 7;13:goaf067. doi: 10.1093/gastro/goaf067. eCollection 2025. Gastroenterol Rep (Oxf). 2025. PMID: 40625657 Free PMC article. Review.
-
Percutaneous mechanical thrombectomy versus catheter-directed thrombolysis for the treatment of arterial acute mesenteric ischemia and risk factors for 30-day mortality.Front Cardiovasc Med. 2025 May 16;12:1553170. doi: 10.3389/fcvm.2025.1553170. eCollection 2025. Front Cardiovasc Med. 2025. PMID: 40454240 Free PMC article.
References
-
- Björck M, Koelemay M, Acosta S, Bastos Goncalves F, Kölbel T, Kolkman JJ, Lees T, Lefevre JH, Menyhei G, Oderich G, et al. Editor's choice—management of the diseases of mesenteric arteries and veins: clinical practice guidelines of the European Society of Vascular Surgery (ESVS). Eur J Vasc Endovasc Surg. 2017;53:460–510. doi: 10.1016/j.ejvs.2017.01.010 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
