

Short-term effects of gastric bypass versus sleeve gastrectomy on high LDL cholesterol: The BASALTO randomized clinical trial
- PMID: 38879559
- PMCID: PMC11180388
- DOI: 10.1186/s12933-024-02296-x
Short-term effects of gastric bypass versus sleeve gastrectomy on high LDL cholesterol: The BASALTO randomized clinical trial
Abstract
Background: There has been a substantial increase in the use of laparoscopic sleeve gastrectomy (SG) to treat morbid obesity despite observational evidence demonstrating the superiority of Roux-en-Y gastric bypass (RYGB) for reducing low-density lipoprotein (LDL) cholesterol. The main aim was to ascertain whether high LDL cholesterol levels should be considered when selecting the most appropriate surgical procedure for each patient (RYGB or SG).
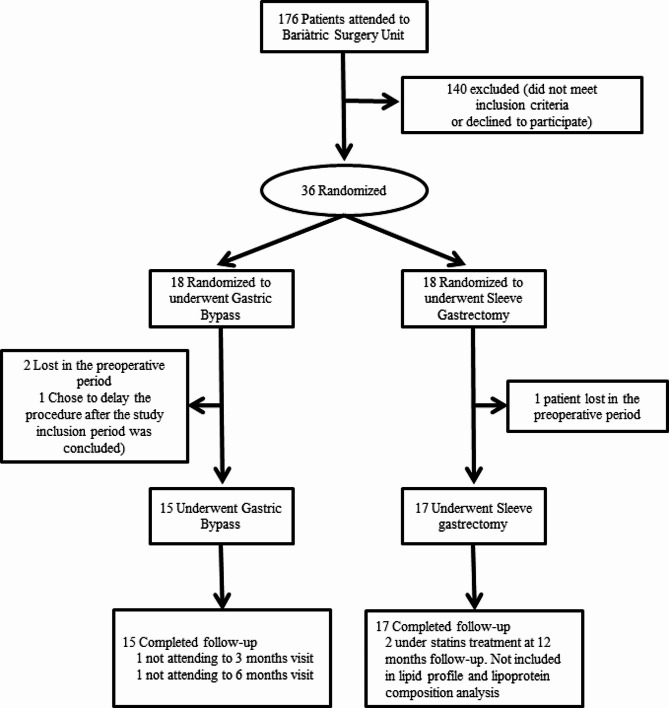
Methods: In this single-center, randomized clinical trial using intention-to-treat analysis, 38 patients with severe obesity and elevated levels of LDL cholesterol were randomly assigned to undergo RYGB or SG. The primary outcome was LDL cholesterol remission at 12 months, defined as LDL cholesterol < 3.36 nmol/l without lipid-lowering medications. Secondary outcomes included changes in weight, other comorbidities, qualitative lipoprotein traits, cholesterol esters, glycoproteins, cholesterol absorption and synthesis metabolites and complications.
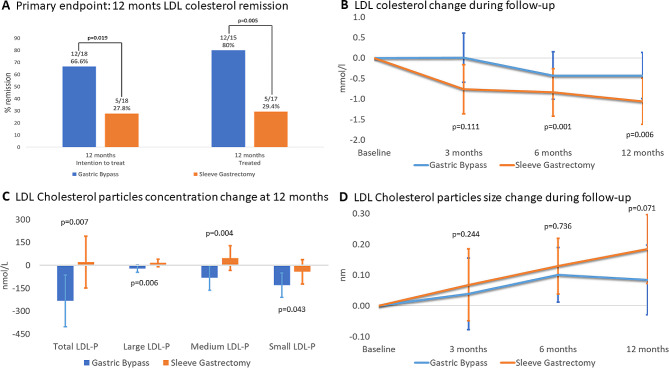
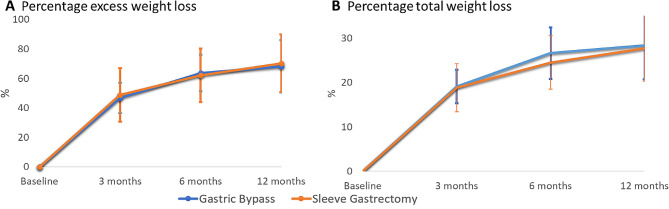
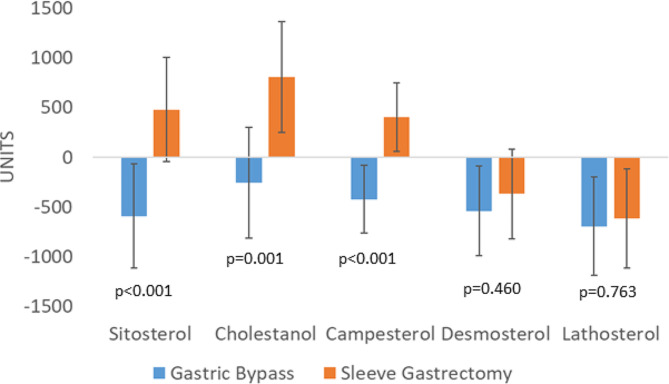
Results: Intention-to-treat analysis revealed that LDL cholesterol remission occurred in 66.6% of RYGB patients compared to 27.8% of SG patients (p = 0.019). Among patients completing follow-up, RYGB demonstrated superior remission (80.0% vs. 29.4%, p = 0.005). Exclusive benefits of RYGB included a reduction in large, medium, and small LDL particles. Cholesterol absorption markers showed differential behavior after both techniques: campesterol (Δ -15.2 µg/mg, 95% CI -30.2 to -0.1) decreased after RYGB, and sitosterol (Δ 21.1 µg/mg, 95% CI 0.9 to 41.2), cholestanol (Δ 30.6 µg/mg, 95% CI 14.8 to 57.9) and campesterol (Δ 18.4 µg/mg, 95% CI 4.4 to 32.3) increased after SG. No differences in weight loss, cholesterol esters, glycoproteins, cholesterol synthesis metabolites or postoperative complications were observed between techniques.
Conclusion: In conclusion, RYGB is superior to SG in terms of short-term of high LDL cholesterol remission. Furthermore, RYGB also led to a greater improvement in lipoprotein parameters that confer an atherogenic profile. Therefore, the presence of elevated levels of LDL cholesterol should be considered when determining the optimal bariatric surgery procedure for each patient.
Trial registration: Clinicaltrials.gov number, NCT03975478).
Keywords: Bariatric surgery; Cholesterol esters; Hypercholesterolemia; LDL cholesterol; Lipoprotein; Roux-en-Y gastric bypass; Sleeve gastrectomy.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Buchwald H, Avidor Y, Braunwald E, Jensen MD, Pories W, Fahrbach K et al. Bariatric surgery: a systematic review and meta-analysis. JAMA [Internet]. 2004 [cited 2016 Jun 13];292:1724–37. http://www.ncbi.nlm.nih.gov/pubmed/15479938. - PubMed
-
- Schiavon CA, Ikeoka DT, De Sousa MG, Silva CRA, Bersch-Ferreira AC, De Oliveira JD, et al. Effects of gastric bypass surgery in patients with hypertension: Rationale and design for a randomised controlled trial (GATEWAY study) BMJ Open. 2014;4:1–8. doi: 10.1136/bmjopen-2014-005702. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- PI19/00006/Instituto de Salud Carlos III (ISCIII) and co-funded by the European Union
- PI19/00006/Instituto de Salud Carlos III (ISCIII) and co-funded by the European Union
- PI19/00006/Instituto de Salud Carlos III (ISCIII) and co-funded by the European Union
- PI19/00006/Instituto de Salud Carlos III (ISCIII) and co-funded by the European Union
LinkOut - more resources
Full Text Sources
Medical
Research Materials
