

Pharmacological treatment of cancer pain and opioid induced nausea and vomiting: online survey and comparison with current guidelines
- PMID: 38879720
- PMCID: PMC11180006
- DOI: 10.1007/s00520-024-08628-7
Pharmacological treatment of cancer pain and opioid induced nausea and vomiting: online survey and comparison with current guidelines
Abstract
Purpose: We assumed that in Palliative Care, even in common clinical situations, the choice of drugs differs substantially between physicians. Therefore, we assessed the practice of pharmaceutical treatment choices of physicians for cancer pain and opioid-induced nausea and vomiting (OINV) and the rationale for their choices.
Methods: An online survey was conducted with physicians covering the following domains: i) Cancer pain therapy: non-opioids in addition to opioids: choice of drug ii) prevention of OINV: choice of drug and mode of application. Current guidelines concerning cancer pain therapy and prevention of OINV were compared.
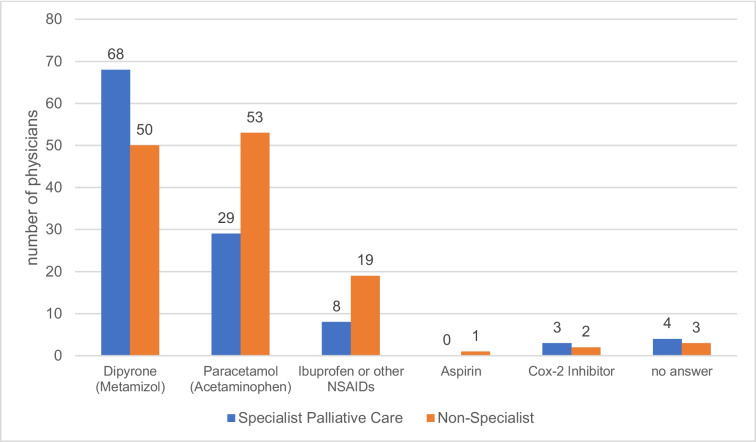
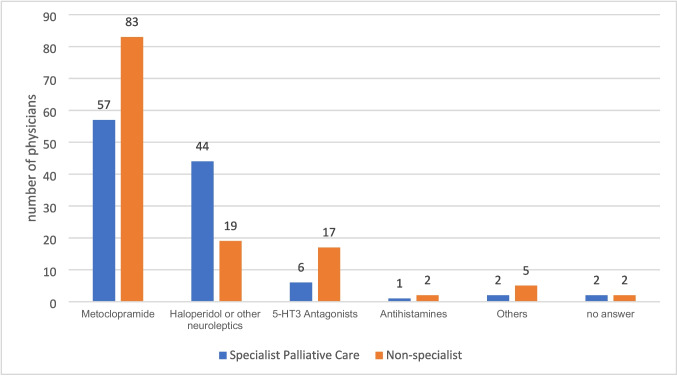
Results: Two-hundred-forty European physicians responded to our survey. i) Use of non-opioids in addition to opioids for the treatment of cancer pain: Only 1.3% (n = 3) of respondents never used an additional non-opioid. Others mostly used: dipyrone/metamizole (49.2%, n = 118), paracetamol/acetaminophen (34.2%, n = 82), ibuprofen / other NSAIDs (11.3%, n = 27), specific Cox2-inhibitors (2.1%, n = 5), Aspirin (0.4%, n = 1), no answer (2.9%, n = 7). ii) Antiemetics to prevent OINV: The drugs of choice were metoclopramide (58.3%, n = 140), haloperidol (26.3%, n = 63), 5-HT3 antagonists (9.6%, n = 23), antihistamines (1.3%, n = 3) and other (2.9%, n = 7); no answer (1.7%, n = 4). Most respondents prescribed the substances on-demand (59.6%, n = 143) while others (36.3%, n = 87) provided them as around the clock medication. Over both domains, most physicians answered that their choices were not based on solid evidence from randomized controlled trials (RCTs). Guidelines were inconsistent regarding if and what non-opioid to use for cancer pain and recommend anti-dopaminergic drugs for prevention or treatment of OINV.
Conclusions: Physician's practice in palliative care for the treatment of cancer pain and OINV differed substantially. Respondents expressed the lack of high-quality evidence- based information from RCTs. We call for evidence from methodologically high-quality RCTs to be available to inform physicians about the benefits and harms of pharmacological treatments for common symptoms in palliative care.
Keywords: Opioid induced nausea and vomiting; Pain management; Palliative care; Pharmacological symptom control; Survey.
© 2024. The Author(s).
Conflict of interest statement
The authors have no relevant financial or non-financial interests to disclose.
Figures
References
-
- WHO Guidelines for the Pharmacological and Radiotherapeutic Management of Cancer Pain in Adults and Adolescents. Geneva: World Health Organization; 2018. 5, Cancer Pain Management – Guiding Principles. Available from: https://www.ncbi.nlm.nih.gov/books/NBK537483/ - PubMed
-
- Siemens W, Boehlke C, Bennett MI, Offner K, Becker G, Gaertner J. Transcutaneous electrical nerve stimulation for advanced cancer pain inpatients in specialist palliative care-a blinded, randomized, sham-controlled pilot cross-over trial. Support Care Cancer. 2020;28(11):5323–5333. doi: 10.1007/s00520-020-05370-8. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
