

Pediatric metabolic (dysfunction)-associated fatty liver disease: current insights and future perspectives
- PMID: 38879851
- PMCID: PMC11450008
- DOI: 10.1007/s12072-024-10691-5
Pediatric metabolic (dysfunction)-associated fatty liver disease: current insights and future perspectives
Abstract
The historical use of the term non-alcoholic fatty liver disease (NAFLD) in obese/overweight children has been controversial as to the appropriateness of this terminology in children, and lately, in adults too. Newer game-changer terminology, metabolic (dysfunction)-associated fatty liver disease (MAFLD), for this condition signifies a positive step forward that addresses the limitations of the previous definition for both adults and children. The prevalence of MAFLD has surged in tandem with the global rise in obesity rates, establishing itself as a predominant cause of chronic liver disease in both adult and pediatric populations. The adoption of the recently proposed nomenclature reflects a more encompassing comprehension of the disease and its etiology compared to its predecessor, NAFLD. Notably, the revised terminology facilitates the recognition of MAFLD as an autonomous condition while acknowledging the potential coexistence of other systemic fatty liver disorders. Particularly in children, this includes various paediatric-onset genetic and inherited metabolic disorders, necessitating thorough exclusion, especially in cases where weight loss interventions yield no improvement or in the absence of obesity. MAFLD presents as a multifaceted disorder; evidence suggests its origins lie in a complex interplay of nutritional, genetic, hormonal, and environmental factors. Despite advancements, current non-invasive diagnostic biomarkers exhibit limitations in accuracy, often necessitating imaging and histological evaluations for definitive diagnosis. While dietary and lifestyle modifications stand as cornerstone measures for MAFLD prevention and management, ongoing evaluation of therapeutic agents continues. This article provides an overview of the latest developments and emerging therapies in the realm of paediatric MAFLD.
Keywords: Adolescents; Children; Diet; Fatty liver disease; Gut microbiome; Lifestyle; Metabolic (dysfunction)-associated fatty liver disease (MAFLD); Non-alcoholic fatty liver disease (NAFLD); Nutrition; Obesity; Weight loss.
© 2024. The Author(s).
Conflict of interest statement
SV, PV and AD declare that they have no conflict of interest. AD sits on the scientific advisory boards for MSD, Alexion, Univar, BitBio, Aspect Bio and Treefrog Bio.
Figures


Similar articles
-
Updates in Metabolic Dysfunction-Associated Fatty Liver Disease (MAFLD) in Children.J Pediatr Gastroenterol Nutr. 2023 Nov 1;77(5):583-591. doi: 10.1097/MPG.0000000000003919. Epub 2023 Aug 18. J Pediatr Gastroenterol Nutr. 2023. PMID: 37592398 Review.
-
Estimating Global Prevalence of Metabolic Dysfunction-Associated Fatty Liver Disease in Overweight or Obese Children and Adolescents: Systematic Review and Meta-Analysis.Int J Public Health. 2021 Oct 6;66:1604371. doi: 10.3389/ijph.2021.1604371. eCollection 2021. Int J Public Health. 2021. PMID: 34690666 Free PMC article.
-
Hepatologists' Awareness and Knowledge of NAFLD and the Familiarity with Renaming NAFLD to MAFLD.Endocr Metab Immune Disord Drug Targets. 2024;24(12):1445-1453. doi: 10.2174/1871530323666221028154159. Endocr Metab Immune Disord Drug Targets. 2024. PMID: 36306455
-
Management of Metabolic-Associated Fatty Liver Disease/Metabolic Dysfunction-Associated Steatotic Liver Disease: From Medication Therapy to Nutritional Interventions.Nutrients. 2024 Jul 11;16(14):2220. doi: 10.3390/nu16142220. Nutrients. 2024. PMID: 39064665 Free PMC article. Review.
-
A Review of the Increasing Prevalence of Metabolic-Associated Fatty Liver Disease (MAFLD) in Children and Adolescents Worldwide and in Mexico and the Implications for Public Health.Med Sci Monit. 2021 Aug 30;27:e934134. doi: 10.12659/MSM.934134. Med Sci Monit. 2021. PMID: 34456329 Free PMC article. Review.
Cited by
-
Epidemiological Dynamics of Burden and Health Inequalities in Metabolic Dysfunction-associated Steatotic Liver Disease in Adolescents at Global, Regional, and National Levels, 1990-2021.J Clin Exp Hepatol. 2025 Jul-Aug;15(4):102537. doi: 10.1016/j.jceh.2025.102537. Epub 2025 Feb 28. J Clin Exp Hepatol. 2025. PMID: 40226388
References
-
- Hegarty R, Deheragoda M, Fitzpatrick E, Dhawan A. Paediatric fatty liver disease (PeFLD): all is not NAFLD - Pathophysiological insights and approach to management. J Hepatol. 2018;68(6):1286–1299 - PubMed
-
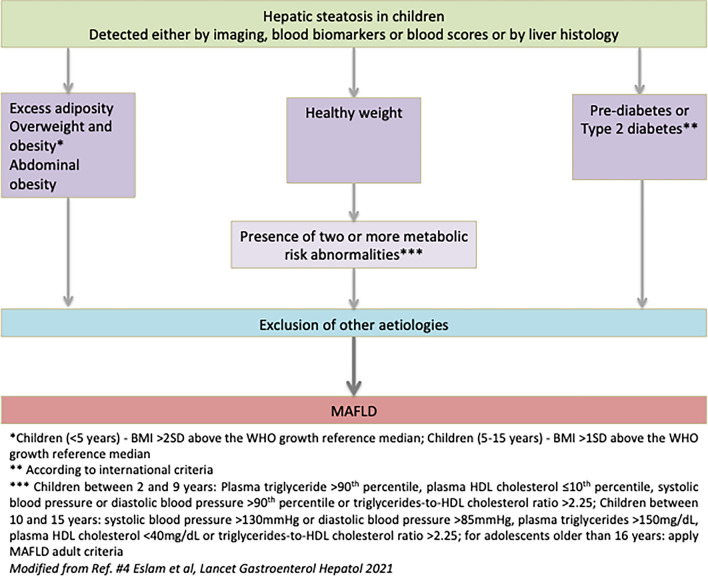
- Eslam M, Alkhouri N, Vajro P, Baumann U, Weiss R, Socha P, et al. Defining paediatric metabolic (dysfunction)-associated fatty liver disease: an international expert consensus statement. Lancet Gastroenterol Hepatol. 2021;6(10):864–873 - PubMed
-
- Kiess W, Penke M, Sergeyev E, Neef M, Adler M, Gausche R, et al. Childhood obesity at the crossroads. J Pediatr Endocrinol Metab. 2015;28(5–6):481–484 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
