

Democratizing FLASH Radiotherapy
- PMID: 38880543
- PMCID: PMC11218907
- DOI: 10.1016/j.semradonc.2024.05.001
Democratizing FLASH Radiotherapy
Abstract
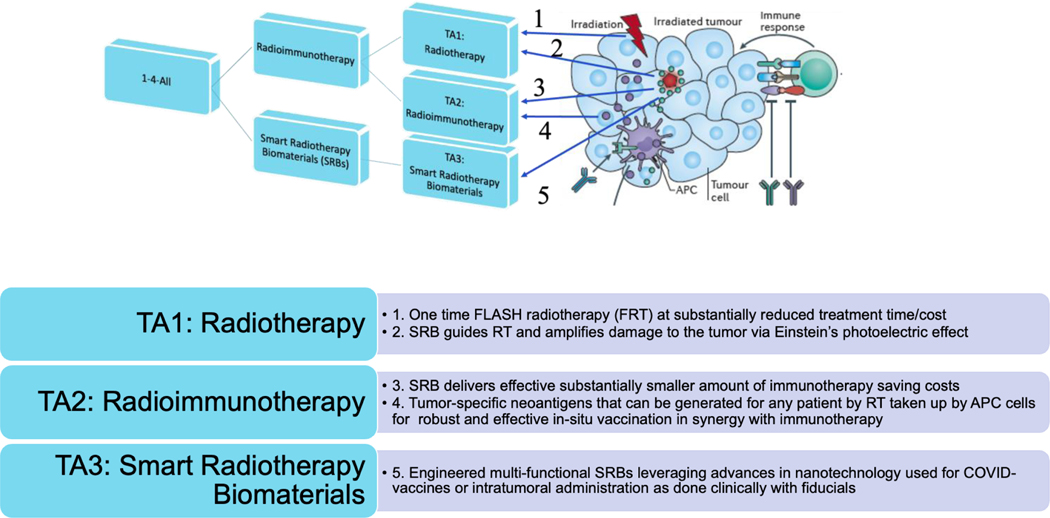
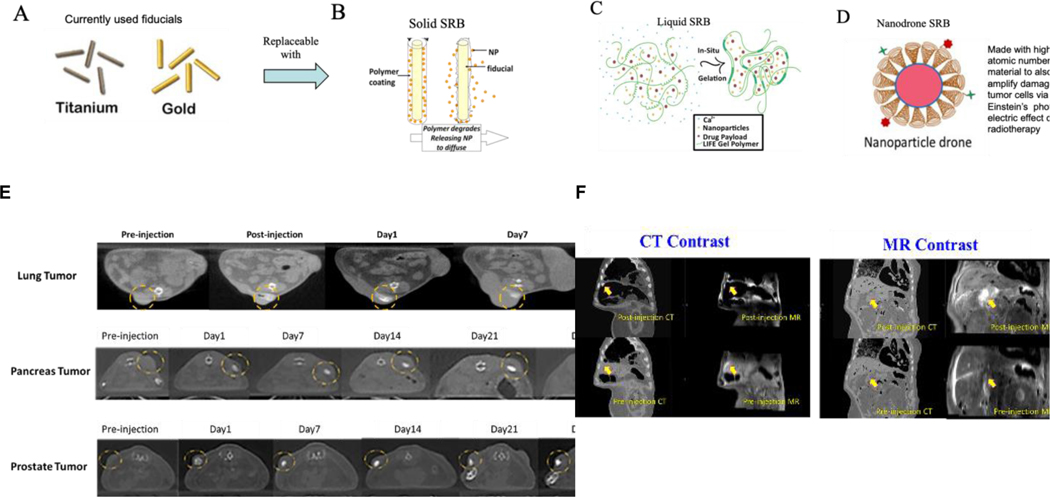
FLASH radiotherapy (RT) is emerging as a potentially revolutionary advancement in cancer treatment, offering the potential to deliver RT at ultra-high dose rates (>40 Gy/s) while significantly reducing damage to healthy tissues. Democratizing FLASH RT by making this cutting-edge approach more accessible and affordable for healthcare systems worldwide would have a substantial impact in global health. Here, we review recent developments in FLASH RT and present perspective on further developments that could facilitate the democratizing of FLASH RT. These include upgrading and validating current technologies that can deliver and measure the FLASH radiation dose with high accuracy and precision, establishing a deeper mechanistic understanding of the FLASH effect, and optimizing dose delivery conditions and parameters for different types of tumors and normal tissues, such as the dose rate, dose fractionation, and beam quality for high efficacy. Furthermore, we examine the potential for democratizing FLASH radioimmunotherapy leveraging evidence that FLASH RT can make the tumor microenvironment more immunogenic, and parallel developments in nanomedicine or use of smart radiotherapy biomaterials for combining RT and immunotherapy. We conclude that the democratization of FLASH radiotherapy represents a major opportunity for concerted cross-disciplinary research collaborations with potential for tremendous impact in reducing radiotherapy disparities and extending the cancer moonshot globally.
Copyright © 2024 The Author(s). Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of competing interest We have no conflicts of interest.
Figures

Similar articles
-
EORTC guidelines for the use of erythropoietic proteins in anaemic patients with cancer: 2006 update.Eur J Cancer. 2007 Jan;43(2):258-70. doi: 10.1016/j.ejca.2006.10.014. Epub 2006 Dec 19. Eur J Cancer. 2007. PMID: 17182241
-
Interventions to reduce acute and late adverse gastrointestinal effects of pelvic radiotherapy for primary pelvic cancers.Cochrane Database Syst Rev. 2018 Jan 23;1(1):CD012529. doi: 10.1002/14651858.CD012529.pub2. Cochrane Database Syst Rev. 2018. PMID: 29360138 Free PMC article.
-
Optimisation of chemotherapy and radiotherapy for untreated Hodgkin lymphoma patients with respect to second malignant neoplasms, overall and progression-free survival: individual participant data analysis.Cochrane Database Syst Rev. 2017 Sep 13;9(9):CD008814. doi: 10.1002/14651858.CD008814.pub2. Cochrane Database Syst Rev. 2017. PMID: 28901021 Free PMC article.
-
Interventions to reduce harm from continued tobacco use.Cochrane Database Syst Rev. 2016 Oct 13;10(10):CD005231. doi: 10.1002/14651858.CD005231.pub3. Cochrane Database Syst Rev. 2016. PMID: 27734465 Free PMC article.
-
A systematic overview of radiation therapy effects in head and neck cancer.Acta Oncol. 2003;42(5-6):443-61. doi: 10.1080/02841860310014886. Acta Oncol. 2003. PMID: 14596506
Cited by
-
FLASH radiotherapy: mechanisms, nanotherapeutic strategy and future development.Nanoscale Adv. 2024 Dec 23;7(3):711-721. doi: 10.1039/d4na00753k. eCollection 2025 Jan 28. Nanoscale Adv. 2024. PMID: 39781242 Free PMC article. Review.
-
Engineered multifunctional nanoparticles for enhanced radiation therapy: three-in-one approach for cancer treatment.Mol Cancer. 2025 Mar 6;24(1):68. doi: 10.1186/s12943-025-02266-1. Mol Cancer. 2025. PMID: 40050802 Free PMC article.
References
-
- Elzawawy A. & Ngwa W. Approaching Global Oncology: The win-win model (IOP Publishing Ltd, Bristol, UK, 2022).
-
- Bray F, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin (2024). - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
