

Targeted therapy for capillary-venous malformations
- PMID: 38880808
- PMCID: PMC11180659
- DOI: 10.1038/s41392-024-01862-9
Targeted therapy for capillary-venous malformations
Abstract
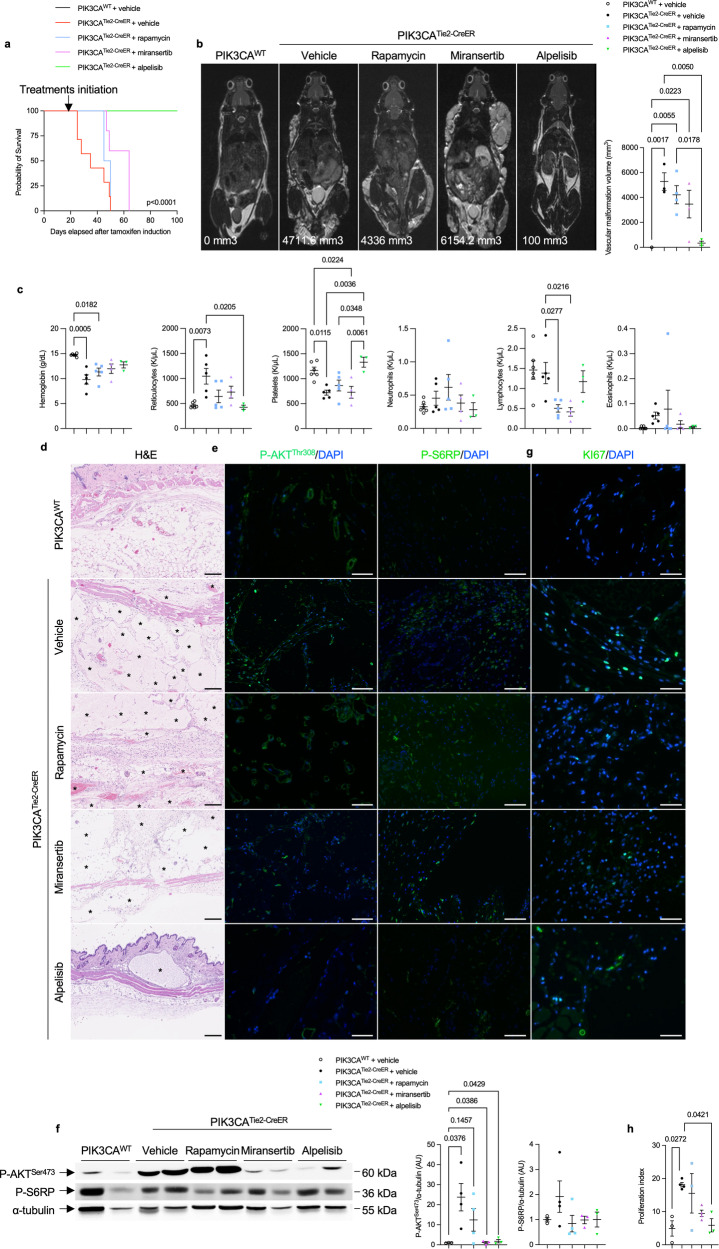
Sporadic venous malformations are genetic conditions primarily caused by somatic gain-of-function mutation of PIK3CA or TEK, an endothelial transmembrane receptor signaling through PIK3CA. Venous malformations are associated with pain, bleedings, thrombosis, pulmonary embolism, esthetic deformities and, in severe cases, life-threatening situations. No authorized medical treatment exists for patients with venous malformations. Here, we created a genetic mouse model of PIK3CA-related capillary venous malformations that replicates patient phenotypes. We showed that these malformations only partially signal through AKT proteins. We compared the efficacy of different drugs, including rapamycin, a mTORC1 inhibitor, miransertib, an AKT inhibitor and alpelisib, a PI3Kα inhibitor at improving the lesions seen in the mouse model. We demonstrated the effectiveness of alpelisib in preventing vascular malformations' occurrence, improving the already established ones, and prolonging survival. Considering these findings, we were authorized to treat 25 patients with alpelisib, including 7 children displaying PIK3CA (n = 16) or TEK (n = 9)-related capillary venous malformations resistant to usual therapies including sirolimus, debulking surgical procedures or percutaneous sclerotherapies. We assessed the volume of vascular malformations using magnetic resonance imaging (MRI) for each patient. Alpelisib demonstrated improvement in all 25 patients. Vascular malformations previously considered intractable were reduced and clinical symptoms were attenuated. MRI showed a decrease of 33.4% and 27.8% in the median volume of PIK3CA and TEK malformations respectively, over 6 months on alpelisib. In conclusion, this study supports PI3Kα inhibition as a promising therapeutic strategy in patients with PIK3CA or TEK-related capillary venous malformations.
© 2024. The Author(s).
Conflict of interest statement
A patent application (“BYL719 (alpelisib) for use in the treatment of PIK3CA-related overgrowth spectrum” #WO2017140828A1) has been filed by INSERM (Institut National de la Santé et de la Recherche Médicale), Centre National De La Recherche Scientifique (CNRS), Université Paris Cité, and Assistance Publique-Hôpitaux De Paris (AP-HP) for the use of BYL719 (alpelisib) in the treatment of
Figures




References
Publication types
MeSH terms
Substances
Grants and funding
- 101000948/EC | EU Framework Programme for Research and Innovation H2020 | H2020 Priority Excellent Science | H2020 European Research Council (H2020 Excellent Science - European Research Council)
- 19-CE14-0030-01/Agence Nationale de la Recherche (French National Research Agency)
- ERC_/European Research Council/International
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Miscellaneous
