Severity of hyperechoic pancreas on preoperative ultrasonography: high potential as a clinically useful predictor of a postoperative pancreatic fistula
- PMID: 38881310
- PMCID: PMC11222128
- DOI: 10.14366/usg.24046
Severity of hyperechoic pancreas on preoperative ultrasonography: high potential as a clinically useful predictor of a postoperative pancreatic fistula
Abstract
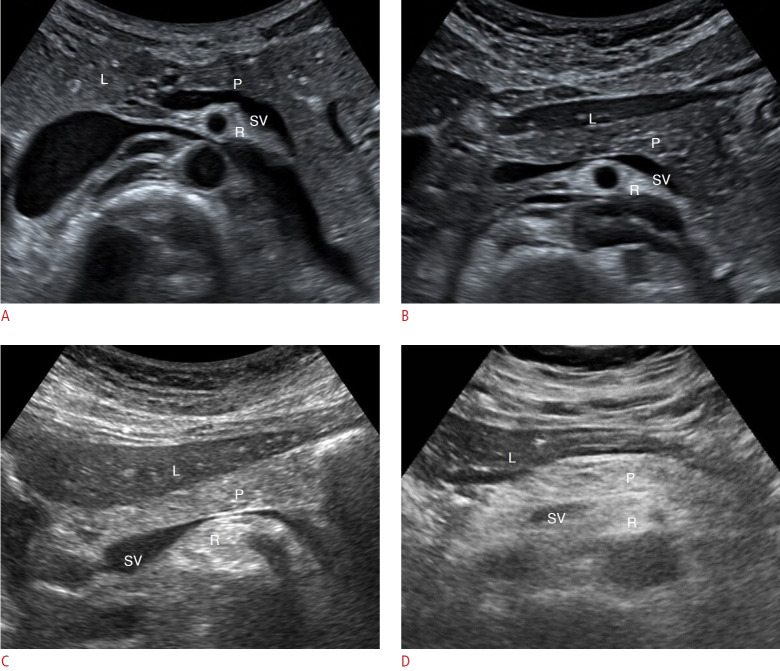
Purpose: This study aimed to evaluate the effectiveness of using the severity of hyperechoic pancreas (HP) observed on preoperative ultrasonography (US) as a predictor of clinically relevant postoperative pancreatic fistula (CR-POPF).
Methods: A retrospective study was conducted with 94 patients who underwent pancreatectomy between April 2006 and March 2021. The severity of HP on US was classified into two categories (normal to mild vs. moderate to severe [obvious HP]). Multiple preoperative and intraoperative parameters were analyzed to predict CR-POPF.
Results: Out of the 94 patients, CR-POPF occurred in 21 (22%) patients, and obvious HP was observed in 30 (32%). Univariate analysis revealed that moderate to severe HP (obvious HP) was significantly associated with an increased incidence of CR-POPF (P<0.001). Factors such as the absence of pancreatitis, a small main pancreatic duct (<3 mm), intraoperative soft pancreas, increased body mass index, and lower pancreatic attenuation and attenuation index were also associated with CR-POPF (all P<0.05). Multivariate analysis showed that obvious HP and soft pancreatic texture were independent predictors of CR-POPF, with odds ratios of 11.53 (P=0.001) and 14.12 (P=0.003), respectively. The combination of obvious HP and soft pancreatic texture provided the most accurate prediction for CR-POPF.
Conclusion: The severity of HP, as observed on preoperative US, was significantly associated with CR-POPF. Severe HP may serve as a clinically useful predictor of POPF, especially when evaluated alongside the intraoperative pancreatic texture.
Keywords: Fatty pancreas; Hyperechoic pancreas; Postoperative pancreatic fistula; Ultrasonography.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures



Similar articles
-
[Use of alternative pancreatic fistula risk score system for patients with clinical relevant postoperative pancreatic fistula after laparoscopic pancreaticoduodenectomy].Zhonghua Wai Ke Za Zhi. 2021 Jul 1;59(7):631-635. doi: 10.3760/cma.j.cn112139-20201026-00766. Zhonghua Wai Ke Za Zhi. 2021. PMID: 34256465 Chinese.
-
Risk Factors for Clinically Relevant Postoperative Pancreatic Fistula (CR-POPF) after Distal Pancreatectomy: A Single Center Retrospective Study.Can J Gastroenterol Hepatol. 2021 Jan 20;2021:8874504. doi: 10.1155/2021/8874504. eCollection 2021. Can J Gastroenterol Hepatol. 2021. PMID: 33542910 Free PMC article.
-
Predictors of Postoperative Pancreatic Fistula (POPF) After Pancreaticoduodenectomy: Clinical Significance of the Mean Platelet Volume (MPV)/Platelet Count Ratio as a New Predictor.J Gastrointest Surg. 2022 Feb;26(2):387-397. doi: 10.1007/s11605-021-05136-5. Epub 2021 Sep 20. J Gastrointest Surg. 2022. PMID: 34545541
-
Risk factors of clinically relevant postoperative pancreatic fistula after pancreaticoduodenectomy: A systematic review and meta-analysis.Medicine (Baltimore). 2022 Jul 1;101(26):e29757. doi: 10.1097/MD.0000000000029757. Medicine (Baltimore). 2022. PMID: 35776984 Free PMC article.
-
Prediction of clinically relevant pancreatic fistula after pancreatic surgery using preoperative CT scan: A systematic review and meta-analysis.Pancreatology. 2020 Oct;20(7):1558-1565. doi: 10.1016/j.pan.2020.09.009. Epub 2020 Sep 12. Pancreatology. 2020. PMID: 32972835
References
-
- Barreto SG, Dirkzwager I, Windsor JA, Pandanaboyana S. Predicting post-operative pancreatic fistulae using preoperative pancreatic imaging: a systematic review. ANZ J Surg. 2019;89:659–665. - PubMed
-
- Roberts KJ, Storey R, Hodson J, Smith AM, Morris-Stiff G. Pre-operative prediction of pancreatic fistula: is it possible? Pancreatology. 2013;13:423–428. - PubMed
-
- Callery MP, Pratt WB, Kent TS, Chaikof EL, Vollmer CM Jr. A prospectively validated clinical risk score accurately predicts pancreatic fistula after pancreatoduodenectomy. J Am Coll Surg. 2013;216:1–14. - PubMed
-
- Lee SE, Jang JY, Lim CS, Kang MJ, Kim SH, Kim MA, et al. Measurement of pancreatic fat by magnetic resonance imaging: predicting the occurrence of pancreatic fistula after pancreatoduodenectomy. Ann Surg. 2010;251:932–936. - PubMed
-
- Ohgi K, Okamura Y, Sugiura T, Ito T, Yamamoto Y, Ashida R, et al. Pancreatic attenuation on computed tomography predicts pancreatic fistula after pancreaticoduodenectomy. HPB (Oxford) 2020;22:67–74. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous