

Food Insecurity and Community-Based Food Resources Among Caregivers of Hospitalized Children
- PMID: 38881356
- PMCID: PMC11208882
- DOI: 10.1542/hpeds.2023-007597
Food Insecurity and Community-Based Food Resources Among Caregivers of Hospitalized Children
Abstract
Objective: Children's hospitals are implementing interventions to connect families to community-based resources. This study describes food insecurity (FI) and food resource knowledge, need, and use among families with a hospitalized child.
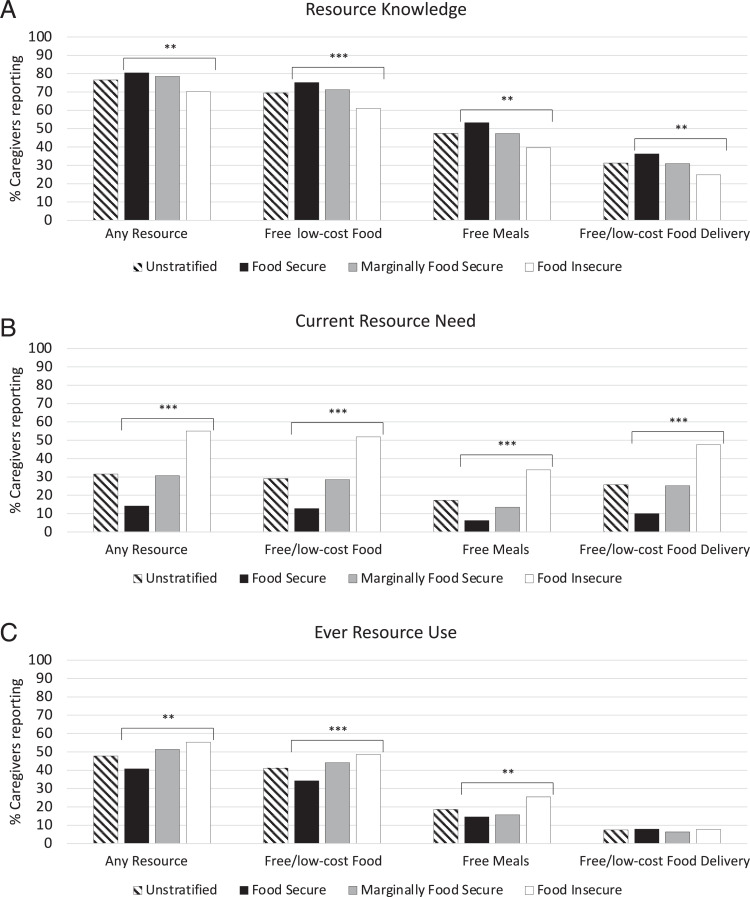
Methods: Between November 2020 and June 2022, 637 caregivers of hospitalized children in an urban 42-ZIP-code area were surveyed as part of a randomized controlled trial. The United States Department of Agriculture 18-item Household Food Security Survey was used to evaluate 12-month food security (food secure [score of 0=FS]; marginally secure [1-2=MFS]; insecure [3-18=FI]). Food resource knowledge, need, and use were described by food security status and examined using Cochran-Armitage tests. The distribution of local resources was obtained from a database and mapped by ZIP code.
Results: Comparing FI (35.0%) with MFS (17.6%) and FS (47.4%) groups, the rates of resource knowledge were lower (70.2% vs 78.5%, 80.5%), and the rates of need (55.1% vs 30.6%, 14.2%) and use (55.3% vs 51.4%, 40.8%) were higher. Rates of food resource knowledge increased linearly with increasing food security (FI to MFS to FS; P = .008), whereas the rates of resource need (P < .001) and use (P = .001) decreased with increasing food security. There were 311 community-based organizations across 36 ZIP codes with participants (range/ZIP code = 0-20, median = 8).
Conclusions: Half of families with a hospitalized child experienced FI or MFS. Although families exhibited high food resource knowledge, nearly half of families with FI had unmet food needs or had never used resources.
Copyright © 2024 by the American Academy of Pediatrics.
Conflict of interest statement
Figures



Comment in
-
Addressing Food Insecurity Among Hospitalized Children: Upstream and Downstream Approaches.Hosp Pediatr. 2024 Jul 1;14(7):e314-e316. doi: 10.1542/hpeds.2024-007807. Hosp Pediatr. 2024. PMID: 38881355 Free PMC article. No abstract available.
References
-
- Coleman-Jensen A, Rabbitt MP, Gregory C, Singh A. Household food security in the United States in 2021. Available at: https://www.ers.usda.gov/webdocs/publications/104656/err-309.pdf. Accessed February 21, 2023
-
- Gundersen C, Ziliak JP. Food insecurity and health outcomes. Health Aff (Millwood). 2015;34(11):1830–1839 - PubMed
-
- Coleman-Jensen A, Rabbitt MP, Gregory CA, Singh A. USDA ERS - household food security in the United States in 2019. Available at: https://www.ers.usda.gov/publications/pub-details/?pubid=99281. Accessed February 21, 2023
-
- Schanzenbach D, Pitts A. Food insecurity during COVID-19 in households with children: results by racial and ethnic groups. Available at: https://www.ipr.northwestern.edu/documents/reports/ipr-rapid-research-re.... Accessed March 4, 2023
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
