

Unraveling Patterns of Congenital Structural Malformations in Infants: A Hospital-Based Descriptive Study
- PMID: 38883135
- PMCID: PMC11178482
- DOI: 10.7759/cureus.60375
Unraveling Patterns of Congenital Structural Malformations in Infants: A Hospital-Based Descriptive Study
Abstract
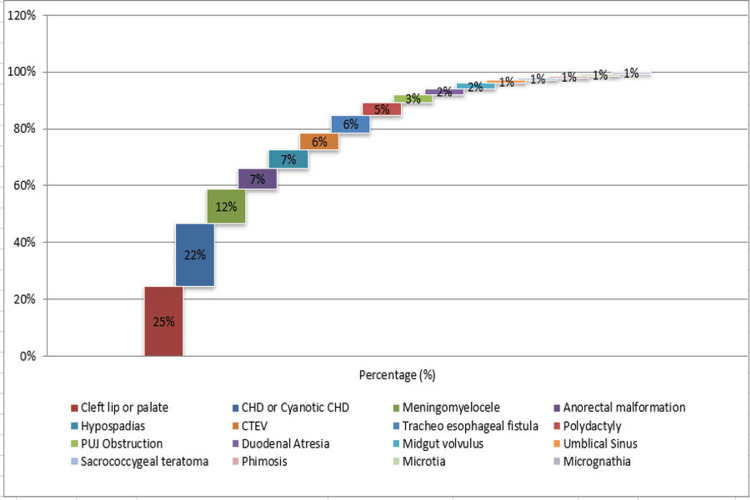
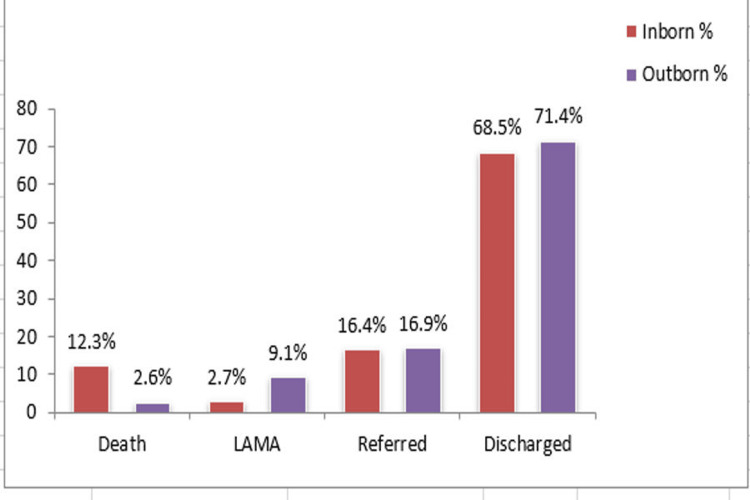
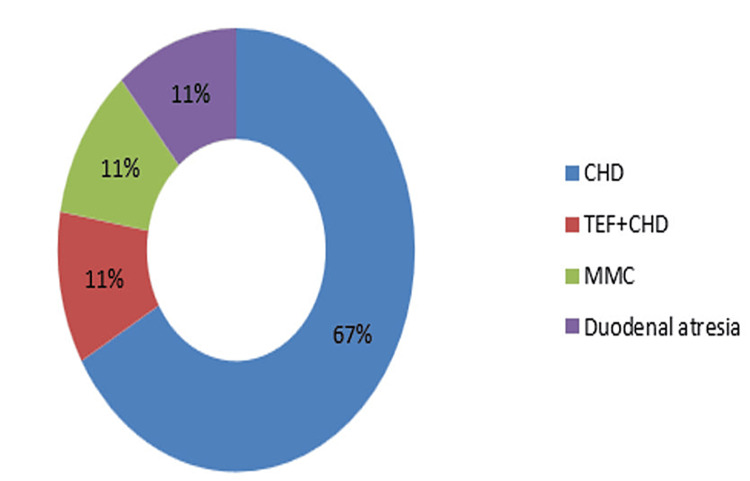
Introduction Congenital malformation studies serve several purposes, including establishing baseline rates, monitoring changes over time, exploring the origins of these defects, and helping in planning health services. Increasing public awareness about pediatric surgical interventions is another goal of these studies. However, the impact of congenital malformations is often underestimated in developing countries due to insufficient healthcare data and diagnostic facilities, particularly in rural areas. Families affected by the birth of a child with congenital malformations face significant stress and hardship. Methods The main aims of this study were to evaluate the clinical pattern of congenital structural malformations in our region (Uttarakhand, India), identify possibly associated factors of congenital malformations, and find out the immediate outcome of congenital malformations in enrolled participants. Results Among a total of 150 cases, 73 (48.7%) cases were inborn, whereas 77 (51.3%) cases were outborn. Investigation of congenital malformation revealed cleft lip or palate in 37 (24.7%) cases, congenital heart disease (CHD) in 33 (22%) cases, meningomyelocele (MMC) in 18 (12.0%) cases, anorectal malformation (ARM) in 11 (7.3%) cases, hypospadias in 10 (6.7%) cases, congenital talipes equinovarus (CTEV) in nine (6.0%) cases, tracheoesophageal fistula (TEF) in nine (6.0%) cases, polydactyly in seven (4.7%) cases, pelviureteric junction obstruction (PUJO) in four (2.7%) cases, duodenal atresia in three (2.0%) cases, midgut volvulus in three (2.0%) cases, umbilical sinus in two (1.3%) cases, sacrococcygeal teratoma (SCT) in one (0.7%) case, phimosis in one (0.7%) case, microtia in one (0.7%) case, and micrognathia in one (0.7%) case. Mortality was observed in 11 (7.3%) cases, whereas 105 (70%) cases were successfully discharged. Among 11 mortality cases, the cause of death was CHD in seven (63.2%) cases, TEF+CHD in two (18.1%) cases, MMC in one (9%) case, and duodenal atresia in one (9%) case. Conclusion Contrary to the common belief that advanced maternal age of greater than 35 years is a major cause, 86.6% of the congenital structural anomalies in our hospital-based study in Uttarakhand occurred in babies of mothers belonging to the age group of 18-30 years. Also, consanguineous marriage was observed in only 3.3% of cases, indicating that it may not be a major contributing factor causing congenital structural malformations in our region. External congenital anomalies are most commonly observed (60.7%), with cleft lip and cleft palate being the most common. The most frequently observed internal congenital anomaly is CHD (22%) followed by gastrointestinal (GI) (18.6%) and urinary anomalies (10.1%). Death and referral are commonly seen in CHD.
Keywords: congenital anomalies; congenital malformations; congenital structural anomalies; external anomalies; internal anomalies.
Copyright © 2024, Pandey et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
[Incidence of congenital heart defects in the Czech Republic--current data].Ceska Gynekol. 2010 May;75(3):221-42. Ceska Gynekol. 2010. PMID: 20731304 Czech.
-
[In utero exposure to benzodiazepine. Is there a risk for anal atresia with lorazepam?].Encephale. 2003 Nov-Dec;29(6):553-9. Encephale. 2003. PMID: 15029090 Review. French.
-
The incidence of congenital anomalies associated with cleft palate/cleft lip and palate in neonates in the Konya region, Turkey.Br J Oral Maxillofac Surg. 2012 Sep;50(6):541-4. doi: 10.1016/j.bjoms.2011.08.001. Epub 2011 Aug 30. Br J Oral Maxillofac Surg. 2012. PMID: 21880407
-
Congenital heart disease and associated malformations in children with cleft lip and palate in Pakistan.Br J Plast Surg. 2003 Mar;56(2):106-9. doi: 10.1016/s0007-1226(03)00044-4. Br J Plast Surg. 2003. PMID: 12791351
-
Clinical and etiological heterogeneity in patients with tracheo-esophageal malformations and associated anomalies.Eur J Med Genet. 2014 Aug;57(8):440-52. doi: 10.1016/j.ejmg.2014.05.009. Epub 2014 Jun 13. Eur J Med Genet. 2014. PMID: 24931924 Review.
References
-
- Congenital anomalies: prevalence and risk factors. Francine R, Pascale S, Aline H. Univers J Public Health. 2014;2:58–63.
-
- Lammens M, Van Vugt JMG, Willemsen M, Van der Voorn JP, Van Bokhoven H, Donkelaar HJ. Clinical Neuroembryology: Development and Developmental Disorders of the Human Central Nervous System. Berlin, Heidelberg: Springer; 2014. Causes of Congenital Malformations.
-
- Perinatal mortality trends in a referral hospital. Kumar MR, Bhat BV, Oumachigui A. Indian J Pediatr. 1996;63:357–361. - PubMed
LinkOut - more resources
Full Text Sources